

Preoperative Visceral Adiposity and Muscularity Predict Poor Outcomes after Hepatectomy for Hepatocellular Carcinoma
- PMID: 31019900
- PMCID: PMC6465724
- DOI: 10.1159/000488779
Preoperative Visceral Adiposity and Muscularity Predict Poor Outcomes after Hepatectomy for Hepatocellular Carcinoma
Abstract
Objective: Visceral adiposity, defined as a high visceral-to-subcutaneous adipose tissue area ratio (VSR), has been shown to be associated with poor outcomes in several cancers. However, in the surgical field, the significance of visceral adiposity remains controversial. The present study investigated the impact of visceral adiposity as well as sarcopenic factors (low muscularity) on outcomes in patients undergoing hepatectomy for hepatocellular carcinoma (HCC).
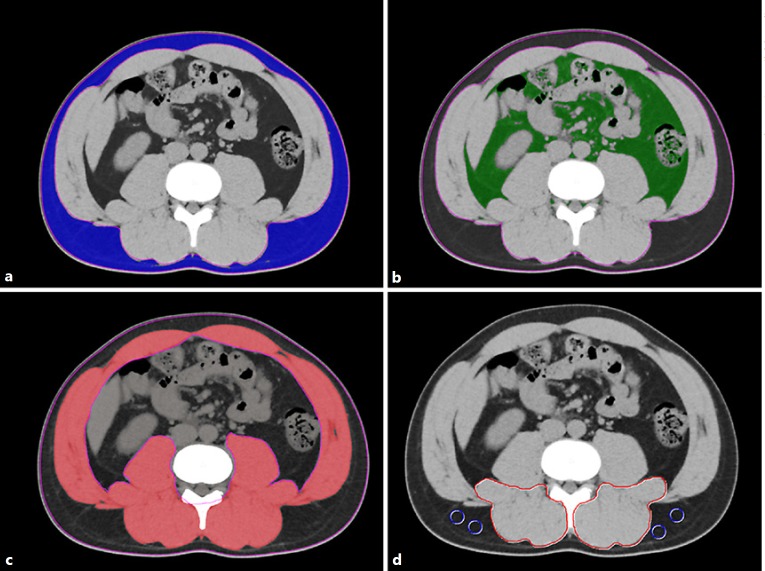
Patients and methods: This retrospective study analyzed data from 606 patients undergoing hepatectomy for HCC at our institution between April 2005 and March 2016. Using preoperative plain computed tomography imaging at the level of the third lumbar vertebra, visceral adiposity, skeletal muscle mass, and muscle quality were evaluated by the VSR, skeletal muscle mass index (SMI), and intramuscular adipose tissue content (IMAC), respectively. The impact of these parameters on outcomes after hepatectomy for HCC was analyzed.
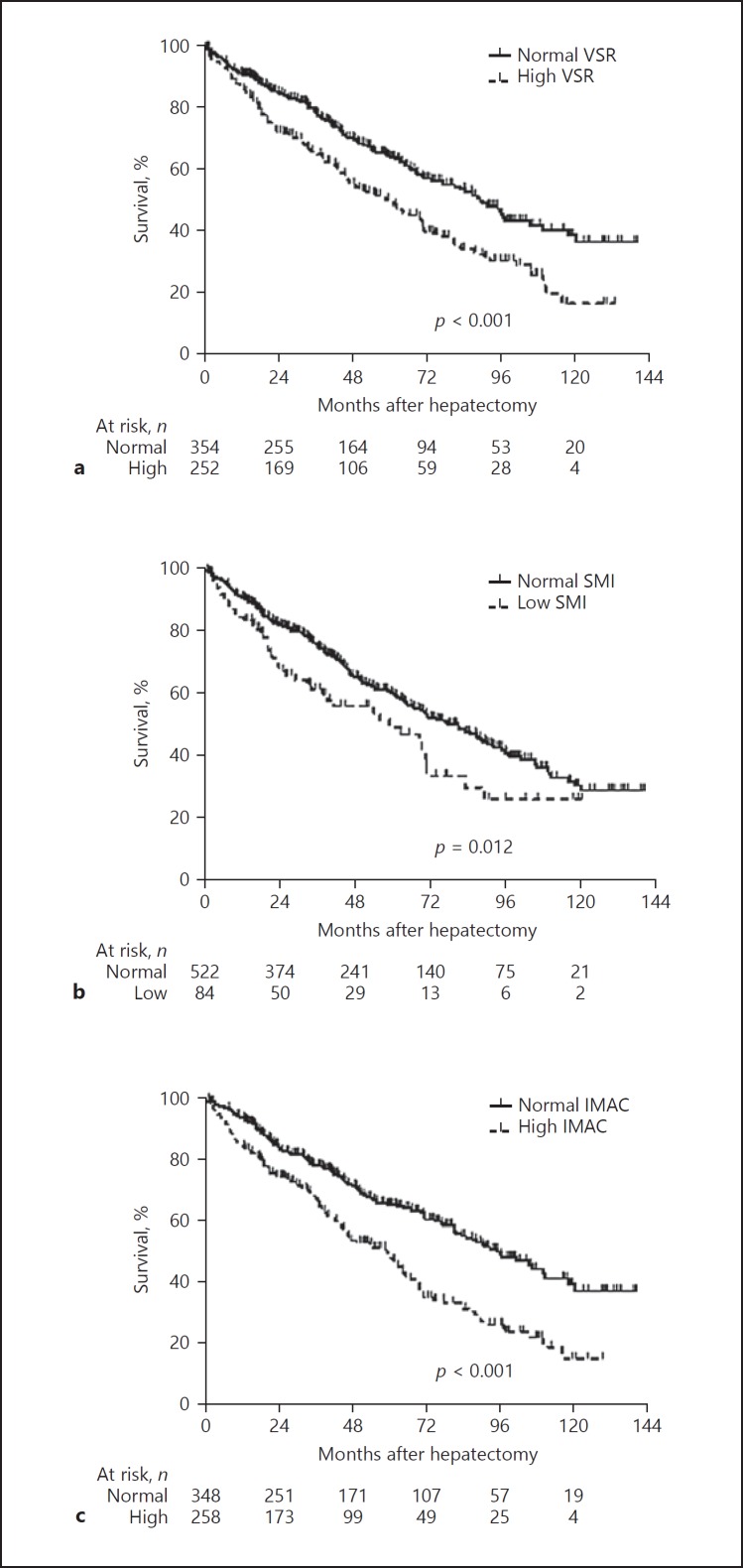
Results: The overall survival rate was significantly lower among patients with a high VSR (p < 0.001) than among patients with a normal VSR. Similarly, the recurrence-free survival rate was significantly lower among patients with a high VSR (p = 0.016). A high VSR, low SMI, and high IMAC contributed to an increased risk of death (p < 0.001) and HCC recurrence (p < 0.001) in an additive manner. Multivariate analysis showed that not only preoperative low muscularity but also visceral adiposity was a significant risk factor for mortality (hazard ratio [HR] = 1.566, p < 0.001) and HCC recurrence (HR = 1.329, p = 0.020) after hepatectomy for HCC.
Conclusions: Preoperative visceral adiposity, as well as low muscularity, was closely related to poor outcomes after hepatectomy for HCC. It is crucial to establish a new strategy including perioperative nutritional interventions with rehabilitation for better outcomes after hepatectomy for HCC.
Keywords: Hepatocellular carcinoma; Intramuscular adipose tissue content; Sarcopenia; Skeletal muscle mass index; Visceral adiposity; Visceral-to-subcutaneous adipose tissue area ratio.
Figures


References
-
- Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245–1255. - PubMed
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sourcesmethods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Llovet JM, Schwartz M, Mazzaferro V. Resection and liver transplantation for hepatocellular carcinoma. Semin Liver Dis. 2005;25:181–200. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
