

Massive Amniotic Fluid Aspiration in a Case of Sudden Neonatal Death With Severe Hypoplasia of the Retrotrapezoid/Parafacial Respiratory Group
- PMID: 31019904
- PMCID: PMC6458245
- DOI: 10.3389/fped.2019.00116
Massive Amniotic Fluid Aspiration in a Case of Sudden Neonatal Death With Severe Hypoplasia of the Retrotrapezoid/Parafacial Respiratory Group
Abstract
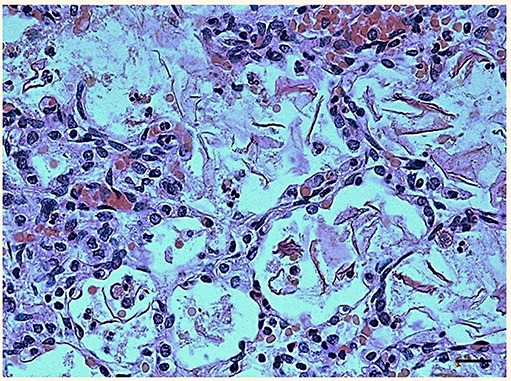
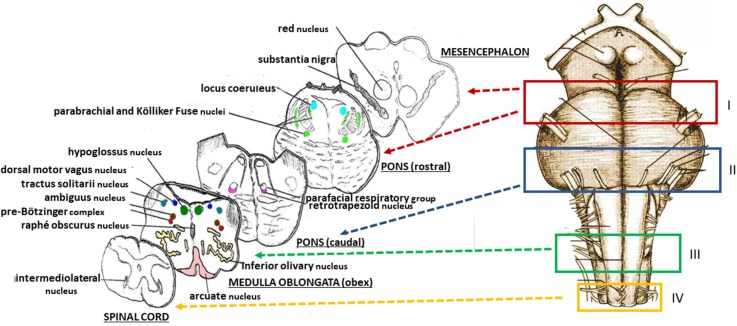
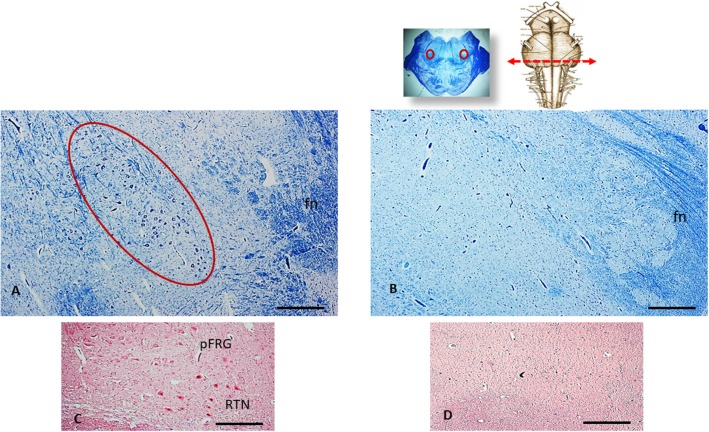
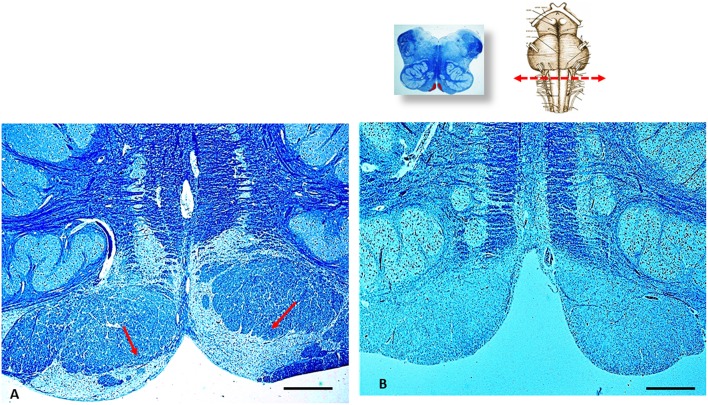
We report a case of a baby, who, after pregnancy complicated by maternal Addison's disease and Hashimoto's thyroiditis and natural delivery, unexpectedly presented a cardiorespiratory collapse and died 1 hour after birth without responding to prolonged neonatal resuscitation maneuvers. The cause of death was reliably established by carrying out a forensic postmortem examination. More specifically, the histological examination of the lungs showed the presence of abundant endoalveolar and endobronchial cornea scales caused by absorption of amniotic fluid. The neuropathological examination of the brainstem highlighted severe hypodevelopment of the retrotrapezoid/parafacial respiratory group, which is a complex of neurons located in the caudal pons that is involved in respiratory rhythm coordination, especially expiration, in conditions of enhanced respiratory drive, as well as in chemoreception. This neuropathological finding shed new light on the mechanisms underlying the massive amniotic fluid aspiration which led to this early death.
Keywords: amniotic fluid inhalation; brainstem; hypoplasia; newborn; retrotrapezoid/parafacial respiratory group; sudden neonatal death.
Figures
Similar articles
-
Amniotic fluid embolism: a cause of sudden maternal death and police inquest.Am J Forensic Med Pathol. 2012 Dec;33(4):330-4. doi: 10.1097/PAF.0b013e31825fb201. Am J Forensic Med Pathol. 2012. PMID: 22835973
-
Neonatal aspiration: not just meconium.J Neonatal Perinatal Med. 2013 Jan 1;6(4):355-7. doi: 10.3233/NPM-1372613. J Neonatal Perinatal Med. 2013. PMID: 24441094
-
Cholinergic modulation of the parafacial respiratory group.J Physiol. 2017 Feb 15;595(4):1377-1392. doi: 10.1113/JP273012. Epub 2016 Dec 11. J Physiol. 2017. PMID: 27808424 Free PMC article.
-
The parafacial respiratory group and the control of active expiration.Respir Physiol Neurobiol. 2019 Jul;265:153-160. doi: 10.1016/j.resp.2018.06.010. Epub 2018 Jun 19. Respir Physiol Neurobiol. 2019. PMID: 29933053 Review.
-
The triple risk hypotheses in sudden infant death syndrome.Pediatrics. 2002 Nov;110(5):e64. doi: 10.1542/peds.110.5.e64. Pediatrics. 2002. PMID: 12415070 Review.
Cited by
-
The Mesencephalic Periaqueductal Gray, a Further Structure Involved in Breathing Failure Underlying Sudden Infant Death Syndrome.ASN Neuro. 2021 Jan-Dec;13:17590914211048260. doi: 10.1177/17590914211048260. ASN Neuro. 2021. PMID: 34623930 Free PMC article.
-
Involvement of the Superior Colliculus in SIDS Pathogenesis.Biomedicines. 2023 Jun 11;11(6):1689. doi: 10.3390/biomedicines11061689. Biomedicines. 2023. PMID: 37371784 Free PMC article.
-
Altered Development of Mesencephalic Dopaminergic Neurons in SIDS: New Insights into Understanding Sudden Infant Death Pathogenesis.Biomedicines. 2021 Oct 26;9(11):1534. doi: 10.3390/biomedicines9111534. Biomedicines. 2021. PMID: 34829763 Free PMC article.
-
New Step in Understanding the Pathogenetic Mechanism of Sudden Infant Death Syndrome: Involvement of the Pontine Reticular Gigantocellular Nucleus.Int J Mol Sci. 2024 Jun 25;25(13):6920. doi: 10.3390/ijms25136920. Int J Mol Sci. 2024. PMID: 39000030 Free PMC article.
-
NBCe1-B/C-knockout mice exhibit an impaired respiratory response and an enhanced renal response to metabolic acidosis.Front Physiol. 2023 Jun 19;14:1201034. doi: 10.3389/fphys.2023.1201034. eCollection 2023. Front Physiol. 2023. PMID: 37405134 Free PMC article.
References
-
- Wright S, Mathieson K, Brearley L, Jacobs S, Holly L, Wickremasinghe R, et al. Ending Newborn Deaths: Ensuring Every Baby Survives. London: Save the Children; (2014). p. 60.
-
- Power G, Blood A. Fetal and neonatal physiology. In: Polin R, Fox W, Abman S. editors. Thermoregulation. Philadelphia, PA: Elsevier; (2011). p. 615–24.
Publication types
LinkOut - more resources
Full Text Sources