

Enhancing Dendritic Cell Therapy in Solid Tumors with Immunomodulating Conventional Treatment
- PMID: 31020037
- PMCID: PMC6475716
- DOI: 10.1016/j.omto.2019.03.007
Enhancing Dendritic Cell Therapy in Solid Tumors with Immunomodulating Conventional Treatment
Abstract
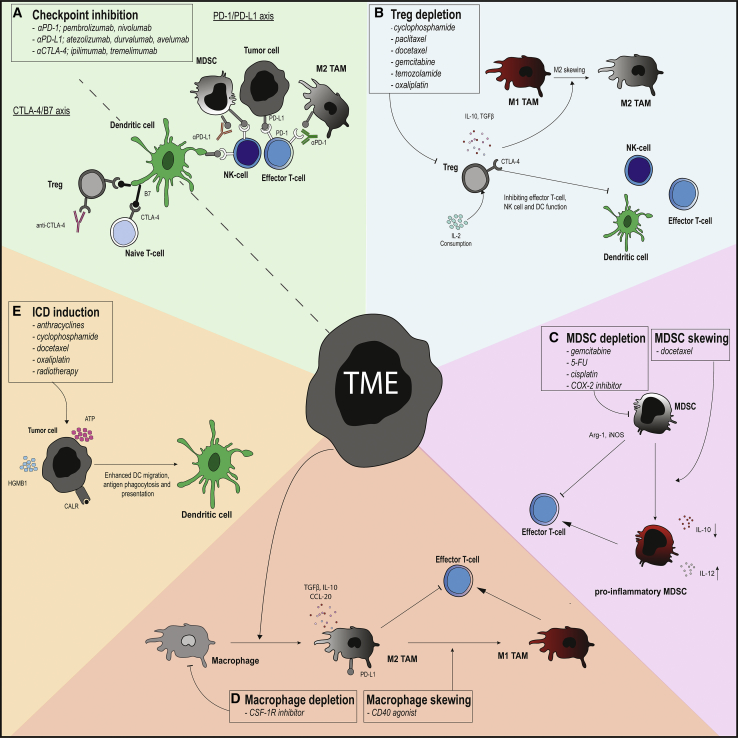
Dendritic cells (DCs) are the most potent antigen-presenting cells and are the key initiator of tumor-specific immune responses. These characteristics are exploited by DC therapy, where DCs are ex vivo loaded with tumor-associated antigens (TAAs) and used to induce tumor-specific immune responses. Unfortunately, clinical responses remain limited to a proportion of the patients. Tumor characteristics and the immunosuppressive tumor microenvironment (TME) of the tumor are likely hampering efficacy of DC therapy. Therefore, reducing the immunosuppressive TME by combining DC therapy with other treatments could be a promising strategy. Initially, conventional cancer therapies, such as chemotherapy and radiotherapy, were thought to specifically target cancerous cells. Recent insights indicate that these therapies additionally augment tumor immunity by targeting immunosuppressive cell subsets in the TME, inducing immunogenic cell death (ICD), or blocking inhibitory molecules. Therefore, combining DC therapy with registered therapies such as chemotherapy, radiotherapy, or checkpoint inhibitors could be a promising treatment strategy to improve the efficacy of DC therapy. In this review, we evaluate various clinical applicable combination strategies to improve the efficacy of DC therapy.
Keywords: checkpoint inhibitors; chemotherapy; dendritic cell-based therapy; immunogenic cell death; immunotherapy; macrophages; myeloid-derived suppressor cells; radiotherapy; regulatory T cells; tumor microenvironment.
Figures
References
-
- Garg A.D., Coulie P.G., Van den Eynde B.J., Agostinis P. Integrating Next-Generation Dendritic Cell Vaccines into the Current Cancer Immunotherapy Landscape. Trends Immunol. 2017;38:577–593. - PubMed
-
- Nace G., Evankovich J., Eid R., Tsung A. Dendritic cells and damage-associated molecular patterns: endogenous danger signals linking innate and adaptive immunity. J. Innate Immun. 2012;4:6–15. - PubMed
-
- Mempel T.R., Henrickson S.E., Von Andrian U.H. T-cell priming by dendritic cells in lymph nodes occurs in three distinct phases. Nature. 2004;427:154–159. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
