

Multivessel spontaneous coronary artery dissection involving the left main coronary artery: a case report
- PMID: 31020244
- PMCID: PMC6439423
- DOI: 10.1093/ehjcr/yty168
Multivessel spontaneous coronary artery dissection involving the left main coronary artery: a case report
Abstract
Background: Spontaneous coronary artery dissection (SCAD) is an infrequent and often misdiagnosis of a non-atherosclerotic cause of acute coronary syndrome (ACS). It is an important cause of ACS in young women, responsible for up to 25% of all cases in women <50 years of age without cardiovascular risk factors. Clinical presentation ranges from ST-segment-elevation myocardial infarction (MI) to ventricular fibrillation and sudden death. The treatment of patients with SCAD is a challenge and the ideal management strategy has yet to be determined.
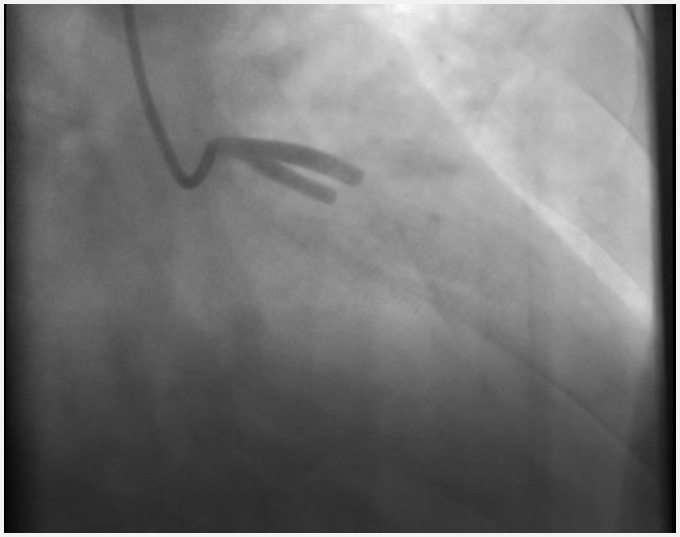
Case summary: A 42-year-old woman without family history of cardiac disease and neither traditional atherosclerotic risk factors presented to our centre with an anterior acute ST-segment-elevation MI secondary to multiple spontaneous dissections of the left main, anterior descending, and ramus intermedius coronary arteries. Stenting was performed in the left anterior descending coronary artery and left main coronary artery to resolve its occlusion. Fibromuscular dysplasia was confirmed via computed tomography angiography.
Discussion: More cases are now being identified of SCAD due to increased clinical index of suspicion, earlier use of invasive angiography, and intracoronary imaging in patients presenting with acute chest pain. Despite this, the absence of previous cardiovascular risk factors and the ignorance of this pathology delay the start of an adequate medical treatment and the performance of a cardiac catheterization. Prognostic data are limited, partly because of its underdiagnosis and lack of prospective studies, so its knowledge is necessary to improve the prognosis of these patients.
Keywords: Acute coronary syndrome; Case report; Fibromuscular dysplasia; Spontaneous coronary artery dissection.
Figures



References
-
- Saw J, Aymong E, Mancini GJ, Sedlak T, Starovoytov A, Ricci D.. Nonatherosclerotic coronary artery disease in young women. Can J Cardiol 2014;30:814–819. - PubMed
-
- Henkin S, Negrotto SM, Tweet MS, Kirmani S, Deyle DR, Gulati R, Olson TM, Hayes SN.. Spontaneous coronary artery dissection and its association with heritable connective tissue disorders. Heart 2016;102:876–881. - PubMed
-
- Vanzetto G, Berger-Coz E, Barone-Rochette G, Chavanon O, Bouvaist H, Hacini R, Blin D, Machecourt J.. Prevalence, therapeutic management and medium-term prognosis of spontaneous coronary artery dissection: results from a database of 11,605 patients. Eur J Cardiothorac Surg 2009;35:250–254. - PubMed
-
- Saw J, Aymong E, Sedlak T, Buller CE, Starovoytov A, Ricci D, Robinson S, Vuurmans T, Gao M, Humphries K, Mancini GBJ.. Spontaneous coronary artery dissection: association with predisposing arteriopathies and precipitating stressors. Circ Cardiovasc Interv 2014;7:645–655. - PubMed
-
- Saw J, Starovoytov A, Humphries K, Sedlak T, Prakash R, Starovoytov A, et al.Canadian Spontaneous Coronary Artery Dissection Cohort Study Oral Session. ESC Congress Munich; 2018, 26 August 2018.
Publication types
LinkOut - more resources
Full Text Sources