

Solitary fibrous tumor in the liver: case report and literature review
- PMID: 31020464
- PMCID: PMC6482201
- DOI: 10.1186/s40792-019-0625-6
Solitary fibrous tumor in the liver: case report and literature review
Abstract
Background: Solitary fibrous tumors (SFTs) are uncommon mesenchymal neoplasms that present most commonly at intrathoracic sites. SFTs of the liver are rare, with only a few having been reported in the English-language literature. We report a rare case of a hepatic SFT and literature review.
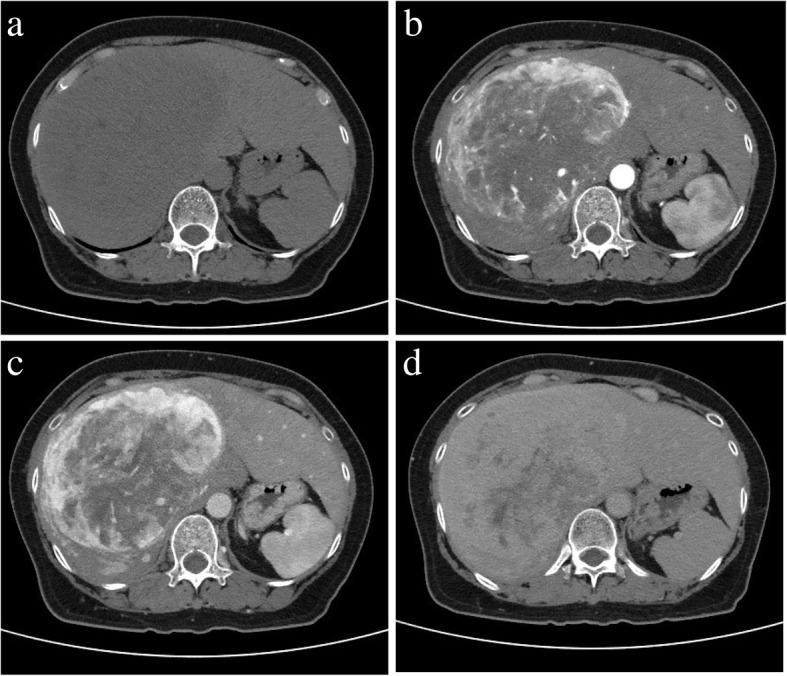
Case presentation: A 49-year-old woman underwent surgery for a cranial hemangiopericytoma two decades previously. She currently presented with malaise. Abdominal computed tomography (CT) showed a huge, sharply demarcated mass in the anterior segment of the liver. Tumor marker levels were within the normal range. Following central bisegmentectomy of the liver, histological examination of the specimen revealed that the tumor was composed of spindle and fibroblast-like cells with collagenous stroma. Immunohistochemically, the spindle cells were negative for CD34 but positive for STAT6. The NAB2-STAT6 fusion gene was detected by the reverse transcription polymerase chain reaction. A diagnosis of SFT was thus confirmed histopathologically and genetically.
Conclusions: The SFT of the liver is an uncommon finding. Because there are no specific imaging features, it is difficult to diagnose the hepatic SFT preoperatively. We consider that careful surgical resection and postoperative follow-up are necessary for hepatic SFTs.
Keywords: Malignant; Radiology and pathology; Solitary fibrous tumor.
Conflict of interest statement
Ethics approval and consent to participate
No applicable.
Consent for publication
Oral informed consent was obtained from the patient for the publication of this case report and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



Similar articles
-
FDG PET/CT and MR imaging of CD34-negative soft-tissue solitary fibrous tumor with NAB2-STAT6 fusion gene.Anticancer Res. 2015 Feb;35(2):967-71. Anticancer Res. 2015. PMID: 25667482
-
A GRIA2 and PAX8-positive renal solitary fibrous tumor with NAB2-STAT6 gene fusion.Diagn Pathol. 2015 Sep 4;10:155. doi: 10.1186/s13000-015-0386-x. Diagn Pathol. 2015. PMID: 26337721 Free PMC article.
-
Molecular characterization of a series of solitary fibrous tumors, including immunohistochemical expression of STAT6 and NATB2-STAT6 fusion transcripts, using Reverse Transcriptase(RT)-Polymerase chain reaction(PCR) technique: An Indian experience.Pathol Res Pract. 2017 Nov;213(11):1404-1411. doi: 10.1016/j.prp.2017.08.011. Epub 2017 Aug 26. Pathol Res Pract. 2017. PMID: 28869107
-
A Rare Case of a Vaginal Solitary Fibrous Tumor, Presenting as a Cystic Mass, Showing NAB2ex4-STAT6ex2 Fusion and STAT6 Immunostaining.Int J Gynecol Pathol. 2019 Jan;38(1):21-26. doi: 10.1097/PGP.0000000000000479. Int J Gynecol Pathol. 2019. PMID: 29257041 Review.
-
'Papillary' solitary fibrous tumor/hemangiopericytoma with nuclear STAT6 expression and NAB2-STAT6 fusion.Brain Tumor Pathol. 2016 Apr;33(2):151-6. doi: 10.1007/s10014-015-0247-z. Epub 2016 Jan 8. Brain Tumor Pathol. 2016. PMID: 26746203 Review.
Cited by
-
A Case of Hepatic Malignant Solitary Fibrous Tumor: A Case Report and Review of the Literature.Case Rep Pathol. 2023 Feb 9;2023:2271690. doi: 10.1155/2023/2271690. eCollection 2023. Case Rep Pathol. 2023. PMID: 36817074 Free PMC article.
-
Solitary fibrous tumor with atypical features of the paravesical space: benign clinical course at the 10-years follow-up. Report of a case and review of the literature.Pathologica. 2020 Dec;112(4):200-209. doi: 10.32074/1591-951X-126. Pathologica. 2020. PMID: 33393523 Free PMC article.
-
Benign focal liver lesions: The role of magnetic resonance imaging.World J Hepatol. 2022 May 27;14(5):923-943. doi: 10.4254/wjh.v14.i5.923. World J Hepatol. 2022. PMID: 35721295 Free PMC article. Review.
-
Vascular tumors of the liver: A brief review.Ann Hepatobiliary Pancreat Surg. 2023 Nov 30;27(4):329-341. doi: 10.14701/ahbps.23-046. Epub 2023 Nov 13. Ann Hepatobiliary Pancreat Surg. 2023. PMID: 37953709 Free PMC article. Review.
-
Cellular solitary fibrous tumor in the mental area: a case report and literature review.J Int Med Res. 2021 Mar;49(3):3000605211000536. doi: 10.1177/03000605211000536. J Int Med Res. 2021. PMID: 33752509 Free PMC article. Review.
References
-
- Fletcher CD, Bridge JA, Lee JC. Extrapleural solitary fibrous tumor. In: Fletcher CD, Bridge JA, Hogendoorn PCW, Mertens F, editors. WHO classification of tumours of soft tissue and bone. fourth ed. Lyon: IARC; 2013. pp. 74–78.
-
- Novais P, Robles-Medranda C, Pannain VL, Barbosa D, Biccas B, Fgaca H. Solitary fibrous liver tumor: is surgical approach the best option? J Gastrointestin Liver Dis. 2010;19:81–84. - PubMed
-
- Chuang IC, Liao KC, Huang HY, Kao YC, Li CF, Huang SC, Tsai JW, Chen KC, Lan J, Lin PC. NAB2-STAT6 gene fusion and STAT6 immunoexpression in extrathoracic solitary fibrous tumors: the association between fusion variants and locations. Pathol Int. 2016;66:288–296. doi: 10.1111/pin.12408. - DOI - PubMed
-
- Robinson DR, Wu YM, Kalyana-Sundaram S, Cao X, Lonigro RJ, Sung YS, Chen CL, Zhang L, Wang R, Su F, Iyer MK, Roychowdhury S, Siddiqui J, Pienta KJ, Kunju LP, Talpaz M, Mosquera JM, Singer S, Schuetze SM, Antonescu CR, Chinnaiyan AM. Identification of recurrent NAB2-STAT6 gene fusions in solitary fibrous tumor by integrative sequencing. Nat Genet. 2013;45:180–185. doi: 10.1038/ng.2509. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
