

Single-Fraction Stereotactic vs Conventional Multifraction Radiotherapy for Pain Relief in Patients With Predominantly Nonspine Bone Metastases: A Randomized Phase 2 Trial
- PMID: 31021390
- PMCID: PMC6487911
- DOI: 10.1001/jamaoncol.2019.0192
Single-Fraction Stereotactic vs Conventional Multifraction Radiotherapy for Pain Relief in Patients With Predominantly Nonspine Bone Metastases: A Randomized Phase 2 Trial
Erratum in
-
Errors in Reported Outcomes and Table.JAMA Oncol. 2021 Oct 1;7(10):1581. doi: 10.1001/jamaoncol.2021.3081. JAMA Oncol. 2021. PMID: 34383015 Free PMC article. No abstract available.
Abstract
Importance: Consensus is lacking as to the optimal radiotherapy dose and fractionation schedule for treating bone metastases.
Objective: To assess the relative efficacy of high-dose, single-fraction stereotactic body radiotherapy (SBRT) vs standard multifraction radiotherapy (MFRT) for alleviation of pain in patients with mostly nonspine bone metastases.
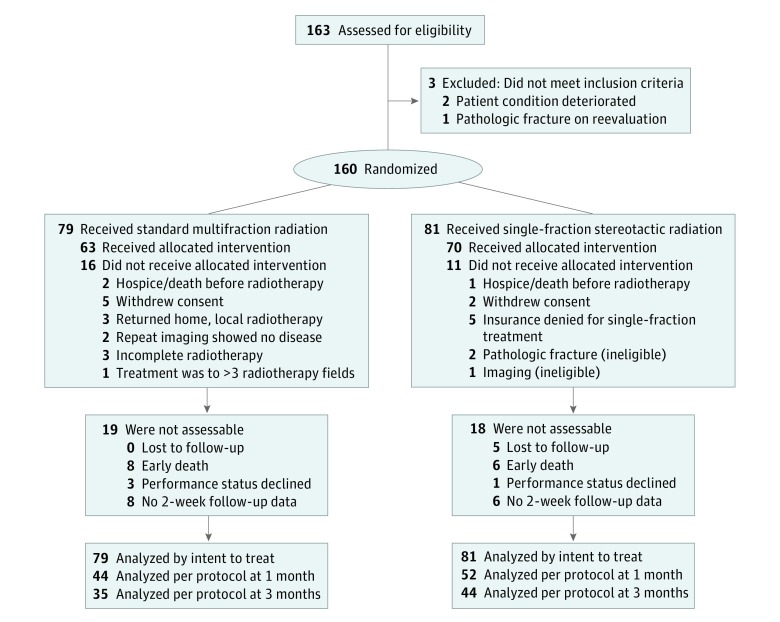
Design, setting, and participants: This prospective, randomized, single-institution phase 2 noninferiority trial conducted at a tertiary cancer care center enrolled 160 patients with radiologically confirmed painful bone metastases from September 19, 2014, through June 19, 2018. Patients were randomly assigned in a 1:1 ratio to receive either single-fraction SBRT (12 Gy for ≥4-cm lesions or 16 Gy for <4-cm lesions) or MFRT to 30 Gy in 10 fractions.
Main outcomes and measures: The primary end point was pain response, defined by international consensus criteria as a combination of pain score and analgesic use (daily morphine-equivalent dose). Pain failure (ie, lack of response) was defined as worsening pain score (≥2 points on a 0-to-10 scale), an increase in morphine-equivalent opioid dose of 50% or more, reirradiation, or pathologic fracture. We hypothesized that SBRT was noninferior to MFRT.
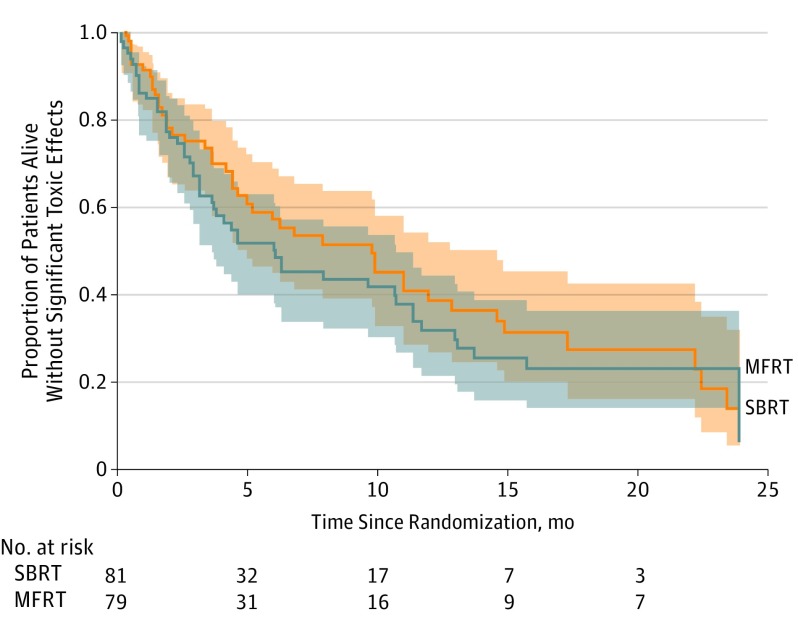
Results: In this phase 2 noninferiority trial of 96 men and 64 women (mean [SD] age, 62.4 [10.4] years), 81 patients received SBRT and 79 received MFRT. Among evaluable patients who received treatment per protocol, the single-fraction group had more pain responders than the MFRT group (complete response + partial response) at 2 weeks (34 of 55 [62%] vs 19 of 52 [36%]) (P = .01), 3 months (31 of 43 [72%] vs 17 of 35 [49%]) (P = .03), and 9 months (17 of 22 [77%] vs 12 of 26 [46%]) (P = .03). No differences were found in treatment-related toxic effects or quality-of-life scores after SBRT vs MFRT; local control rates at 1 and 2 years were higher in patients receiving single-fraction SBRT.
Conclusions and relevance: Delivering high-dose, single-fraction SBRT seems to be an effective treatment option for patients with painful bone metastases. Among evaluable patients, SBRT had higher rates of pain response (complete response + partial response) than did MFRT and thus should be considered for patients expected to have relatively long survival.
Trial registration: ClinicalTrials.gov identifier: NCT02163226.
Conflict of interest statement
Figures

Comment in
-
Single-fraction radiotherapy for bone metastases.Lancet Oncol. 2019 Jun;20(6):e296. doi: 10.1016/S1470-2045(19)30282-7. Epub 2019 May 3. Lancet Oncol. 2019. PMID: 31060792 No abstract available.
-
Errors in Reported Primary and Secondary Outcomes and Table Numbers in a Trial of Radiotherapy for Pain Relief in Patients With Bone Metastases.JAMA Oncol. 2021 Oct 1;7(10):1576-1577. doi: 10.1001/jamaoncol.2021.3054. JAMA Oncol. 2021. PMID: 34383007 No abstract available.
References
-
- Wu JS, Wong R, Johnston M, Bezjak A, Whelan T; Cancer Care Ontario Practice Guidelines Initiative Supportive Care Group . Meta-analysis of dose-fractionation radiotherapy trials for the palliation of painful bone metastases. Int J Radiat Oncol Biol Phys. 2003;55(3):594-605. doi:10.1016/S0360-3016(02)04147-0 - DOI - PubMed
