

Central nervous system melioidosis: A systematic review of individual participant data of case reports and case series
- PMID: 31022232
- PMCID: PMC6504113
- DOI: 10.1371/journal.pntd.0007320
Central nervous system melioidosis: A systematic review of individual participant data of case reports and case series
Abstract
Background: Central nervous system (CNS) melioidosis is rare. However, delayed diagnosis and treatment could lead to fatality. To identify knowledge of CNS melioidosis, we systematically review case reports and case series.
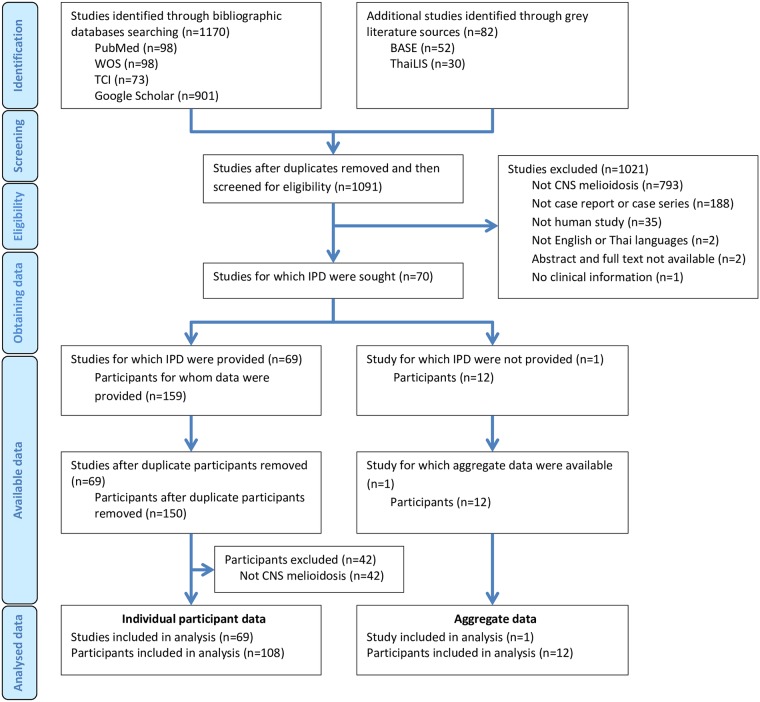
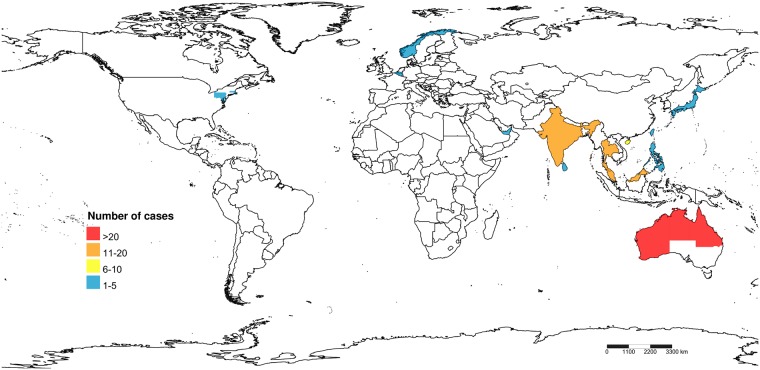
Methodology/principal findings: We searched through PubMed, Web of Science and Thai-Journal Citation Index databases as well as Google Scholar with the last date on July 10, 2018. The diagnosis of CNS melioidosis had to be confirmed with culture, serology or polymerase chain reaction. We excluded the animal cases and the studies that the clinical data were not available. We identified 1170 relevant studies, while 70 studies with a total of 120 patients were analyzed. Ninety-three percent of patients were reported from the endemic area of melioidosis. Median age was 40 years (IQR 18-53), and 70% were men. A total of 60% had one or more risk factors for melioidosis. The median duration from clinical onset to diagnosis was ten days (IQR 5-25). Fever (82%), headache (54%), unilateral weakness (57%) and cranial nerve deficits (52%) are among the prominent presentation. Most patient (67%) had at least one extraneurological organ involvement. The CSF profile mostly showed mononuclear pleocytosis (64%), high protein (93%) and normal glucose (66%). The rim-enhancing pattern (78%) is the most frequent neuroimaging finding in encephalomyelitis and brain abscess patients. Both brainstem (34%) and frontal lobe (34%) are the most affected locations. Mortality rate was 20%.
Conclusions/significance: This study is the most extensive systematic review of case reports and case series of CNS melioidosis in all age groups. However, the results should be cautiously interpreted due to the missing data issue. The propensity of brainstem involvement which correlates with prominent cranial nerve deficits is the characteristic of CNS melioidosis especially encephalomyelitis type. The presenting features of fever and neurological deficits (especially cranial nerve palsies) along with the mononuclear CSF pleocytosis in a patient who lives in the endemic area and also has the risk factor for melioidosis should raise the CNS melioidosis as the differential diagnosis.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: MW reports grants from the Faculty of Medicine, Srinakharinwirot University and HRH Princess Maha Chakri Sirindhorn Medical Center during the conduct of the study. PL declares no competing interests.
Figures
References
-
- Limmathurotsakul D, Chaowagul W, Wongsrikaew P, Narmwong A, Day NP, Peacock SJ. Variable presentation of neurological melioidosis in Northeast Thailand. Am J Trop Med Hyg. 2007; 77: 118–120. - PubMed
-
- Prasad GL, Kini P, Divya S. Central nervous system melioidosis in the pediatric age group. Childs Nerv Syst. 2017; 33: 1–6. - PubMed
-
- Beck RW, Janssen RS, Smiley ML, Schatz NJ, Savino PJ, Rubin DH. Melioidosis and bilateral third-nerve palsies. Neurology. 1984; 34: 105–107. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
