

Effectiveness and Safety of Direct Oral Anticoagulants versus Vitamin K Antagonists for People Aged 75 Years and over with Atrial Fibrillation: A Systematic Review and Meta-Analyses of Observational Studies
- PMID: 31022899
- PMCID: PMC6518135
- DOI: 10.3390/jcm8040554
Effectiveness and Safety of Direct Oral Anticoagulants versus Vitamin K Antagonists for People Aged 75 Years and over with Atrial Fibrillation: A Systematic Review and Meta-Analyses of Observational Studies
Abstract
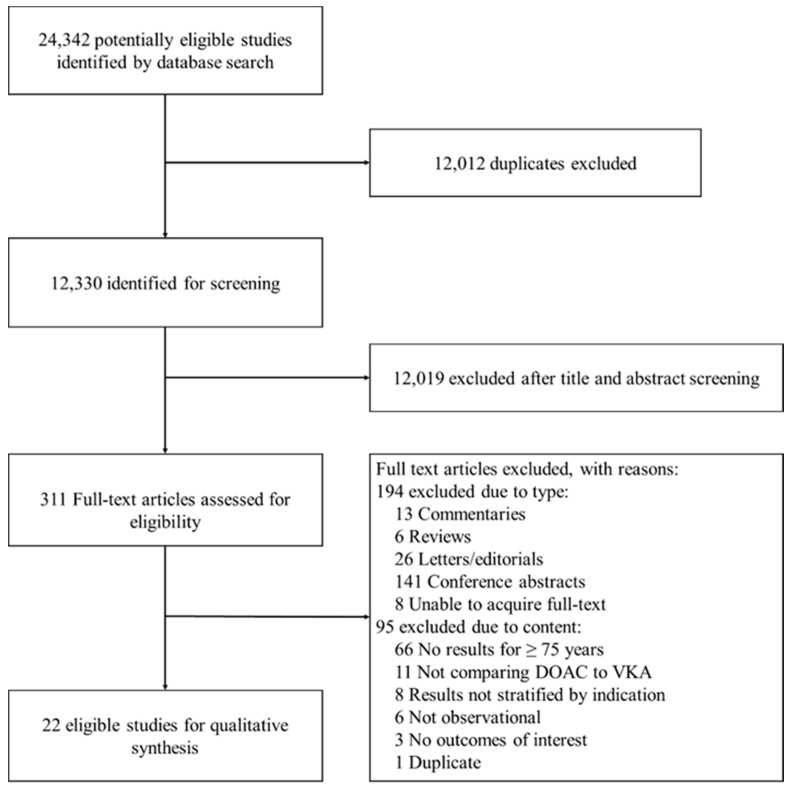
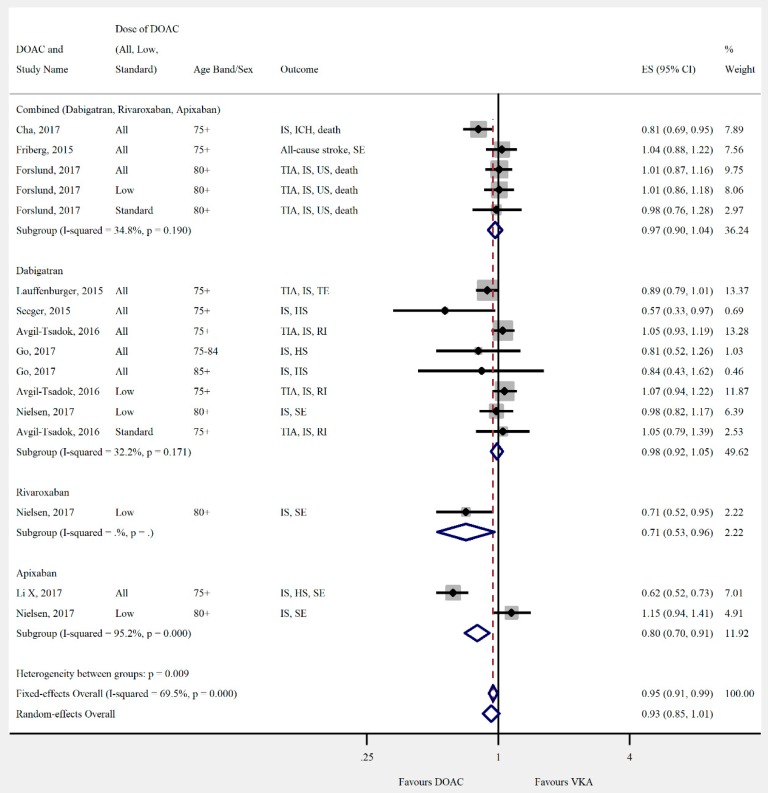
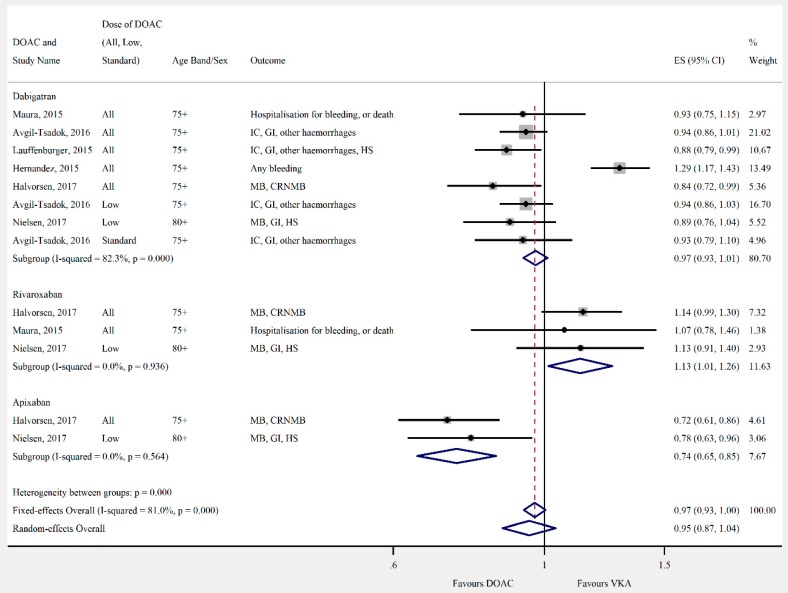
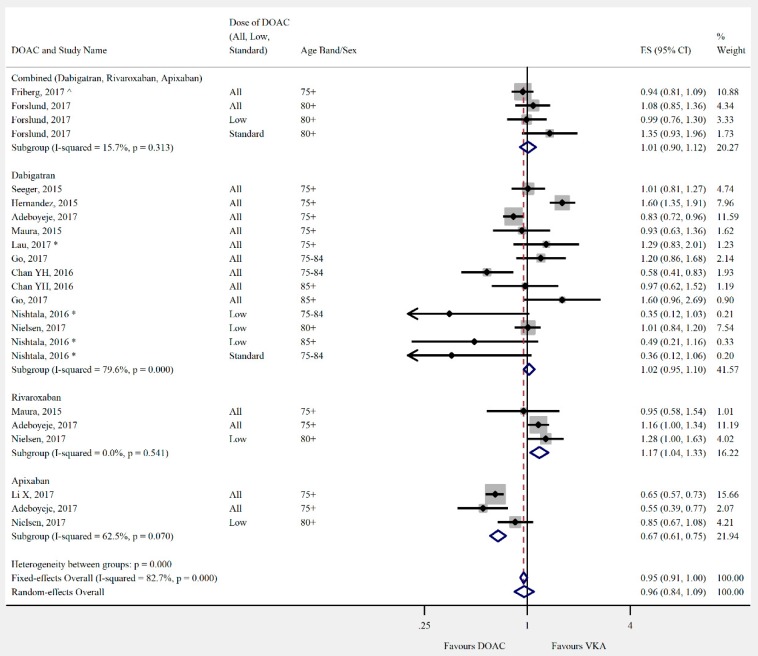
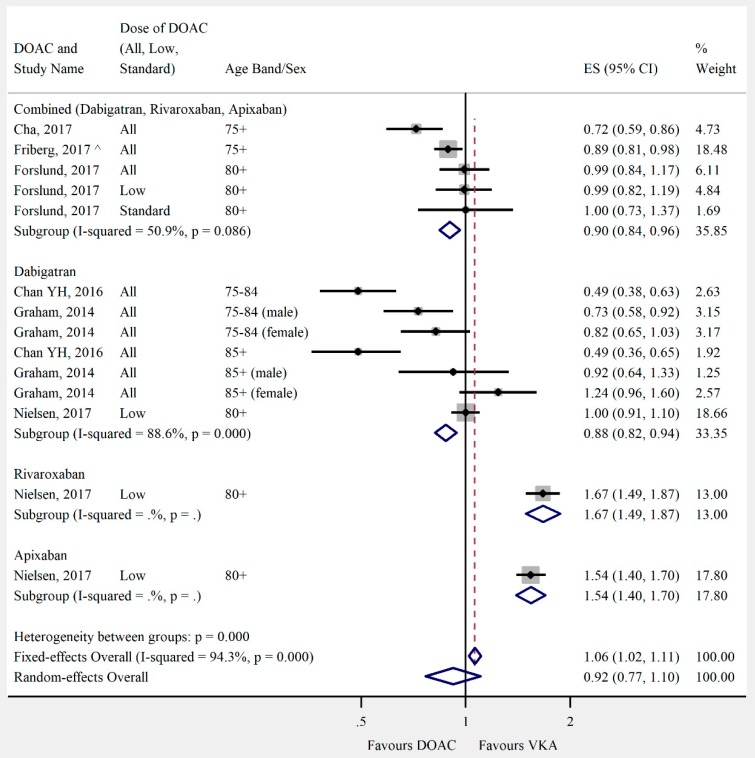
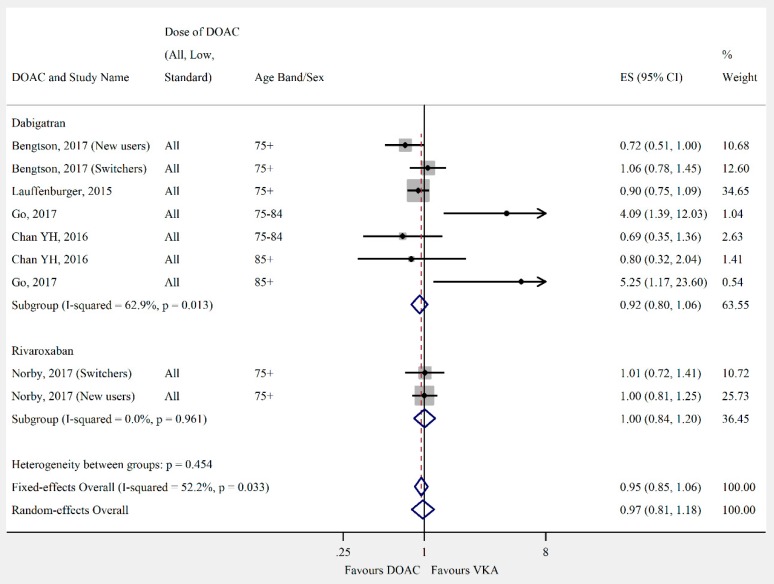
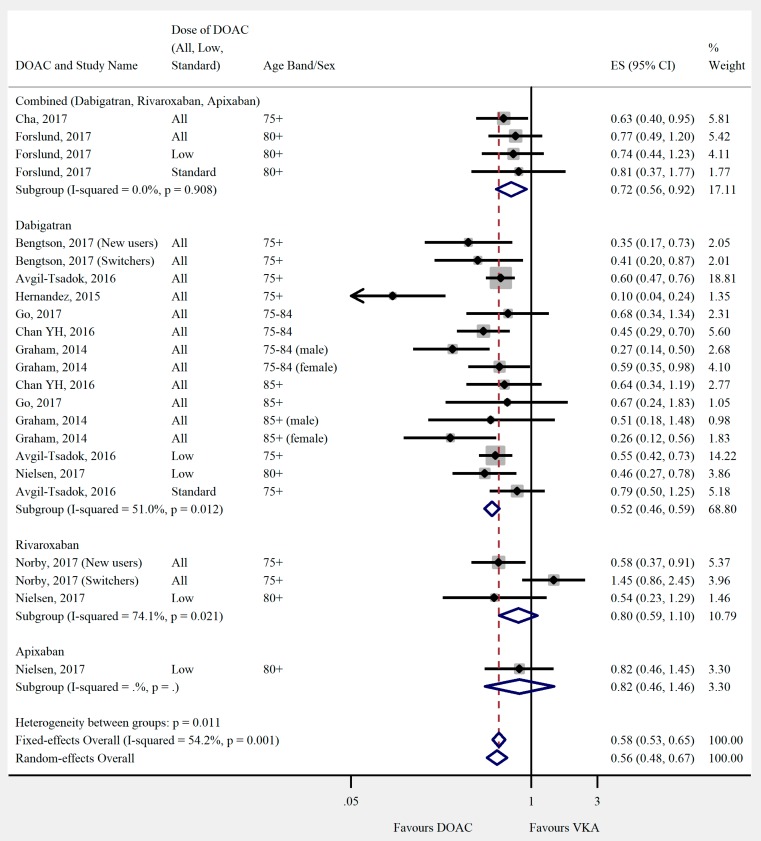
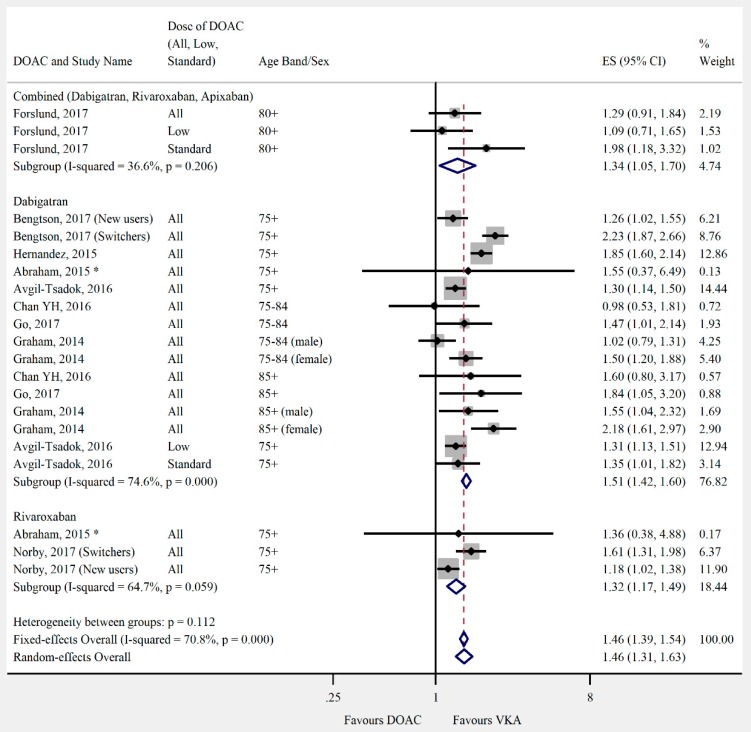
Older people, are underrepresented in randomised controlled trials of direct oral anticoagulants (DOACs) for stroke prevention in atrial fibrillation (AF). The aim of this study was to combine data from observational studies to provide evidence for the treatment of people aged ≥75 years. Medline, Embase, Scopus and Web of Science were searched. The primary effectiveness outcome was ischaemic stroke. Safety outcomes were major bleeding, intracranial haemorrhage, gastrointestinal bleeding, myocardial infarction, and mortality. Twenty-two studies were eligible for inclusion. Two studies related specifically to people ≥75 years but were excluded from meta-analysis due to low quality; all data in the meta-analyses were from subgroups. The pooled risk estimate of ischaemic stroke was slightly lower for DOACs. There was no significant difference in major bleeding, mortality, or myocardial infarction. Risk of intracranial haemorrhage was 44% lower with DOACs, but risk of GI bleeding was 46% higher. Our results suggest that DOACs may be preferable for the majority of older patients with AF, provided they are not at significant risk of a GI bleed. However, these results are based entirely on data from subgroup analyses so should be interpreted cautiously. There is a need for adequately powered research in this patient group.
Keywords: aged; anticoagulants; atrial fibrillation; hemorrhage; stroke.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures

References
-
- Mant J., Hobbs F.D., Fletcher K., Roalfe A., Fitzmaurice D., Lip G.Y., Murray E. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged Study, BAFTA): A randomised controlled trial. Lancet. 2007;370:493–503. doi: 10.1016/S0140-6736(07)61233-1. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
