

Resistant hypertension and cardiovascular disease mortality in the US: results from the National Health and Nutrition Examination Survey (NHANES)
- PMID: 31023262
- PMCID: PMC6485047
- DOI: 10.1186/s12882-019-1315-0
Resistant hypertension and cardiovascular disease mortality in the US: results from the National Health and Nutrition Examination Survey (NHANES)
Abstract
Background: Apparent treatment-resistant hypertension (aTRH) is a common condition associated with risk of cardiovascular events. However, the risk of cardiovascular mortality associated with aTRH in the US population is unknown. We aimed to assess the risk of cardiovascular disease (CVD) mortality associated with aTRH in the US population.
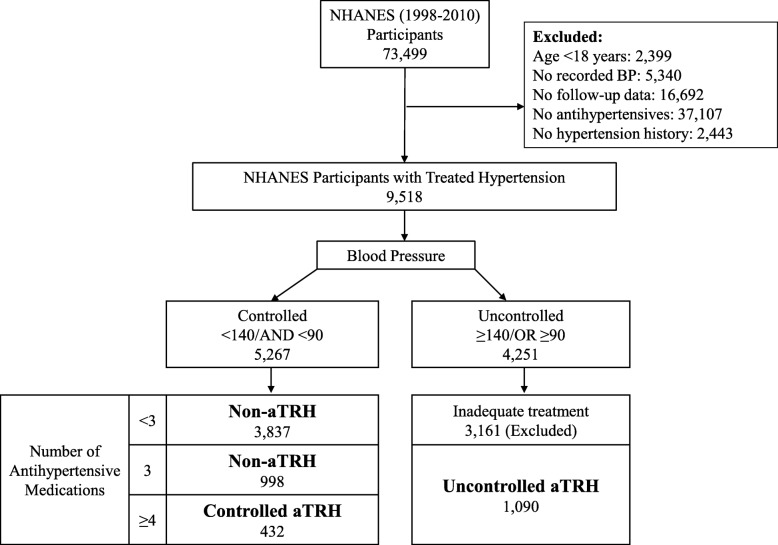
Methods: We analyzed data from 6357 adult hypertensive participants of the National Health and Nutrition Examination Survey (1988-1994 and 1999-2010) linked to the National Death Index. Based on presence of uncontrolled hypertension [blood pressure (BP) ≥140/90 mmHg] and the number of antihypertensives prescribed, we classified participants into the following groups: non-aTRH (BP < 140/90 mmHg and ≤ 3 antihypertensives); controlled aTRH (BP < 140/90 mmHg and ≥ 4 antihypertensives); and uncontrolled aTRH (BP ≥140/90 mmHg and ≥ 3 antihypertensives).
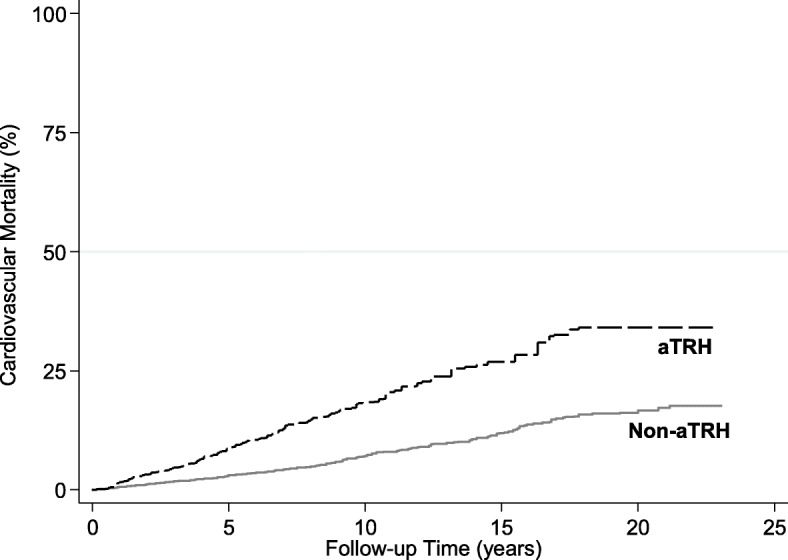
Results: Of the 6357 participants, 1522 had aTRH, representing a US prevalence of 7.6 million. Of the participants with aTRH, 432 had controlled aTRH and 1090 had uncontrolled aTRH. During follow-up (median 6 years), there were 550 CVD deaths. The cumulative incidence of CVD mortality was significantly higher in the aTRH group compared with non-aTRH group (log-rank p < 0.001). In fully adjusted models, aTRH was associated with a 47% higher risk of CVD mortality compared with the non-aTRH group [1.47 (1.1-1.96)]. Similar increase in risk of CVD mortality was noted across aTRH subgroups compared with the non-aTRH group: controlled aTRH [1.66 (1.03-2.68)] and uncontrolled aTRH [1.43 (1.05-1.94)]. Among non-aTRH subgroups, those on 3 antihypertensive medications had a 35% increased risk of CVD mortality than those on < 3 medications [1.35 (0.98-1.86)].
Conclusions: aTRH is a common condition, affecting approximately 7.6 million Americans. Regardless of BP control, people with aTRH remain at a higher risk of cardiovascular outcomes. The risk of cardiovascular disease mortality remains high among those with controlled BP on 3 medications (non-aTRH) or ≥ 4 medications (controlled aTRH), groups not generally considered at high risk. Future risk reduction interventions should consider focusing on these high-risk groups.
Keywords: All-cause mortality; Anti-hypertensives; Cardiovascular mortality; Hypertension.
Conflict of interest statement
Ethics approval and consent to participate
The protocols for conduct of NHANES were approved by the NCHS institutional review board and written informed consent was obtained from all participants. The Johns Hopkins Medical Institutions Institutional Review Board reviewed and approved the study.
Consent for publication
Not applicable.
Competing interests
Tariq Shafi is an Editorial Board Member of BMC Nephrology.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Yoon SS, Carroll MD, Fryar CD. Hypertension prevalence and control among adults: United states, 2011-2014. NCHS data brief. 2015. pp. 1–8. - PubMed
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA, Godwin J, Qizilbash N, Taylor JO, Hennekens CH. Blood pressure, stroke, and coronary heart disease. Part 2, short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827–838. doi: 10.1016/0140-6736(90)90944-Z. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
