

Long-term effects of motherfit group therapy in pre-(MOTHERFIT1) and post-partum women (MOTHERFIT2) with stress urinary incontinence compared to care-as-usual: study protocol of two multi-centred, randomised controlled trials
- PMID: 31023381
- PMCID: PMC6485130
- DOI: 10.1186/s13063-019-3331-6
Long-term effects of motherfit group therapy in pre-(MOTHERFIT1) and post-partum women (MOTHERFIT2) with stress urinary incontinence compared to care-as-usual: study protocol of two multi-centred, randomised controlled trials
Abstract
Background: Stress urinary incontinence (SUI) is highly prevalent during pregnancy and after delivery. It is often associated with a failing pelvic floor, sphincteric and/or supportive system. Pelvic-floor-muscle training (PFMT) peri-partum has been proven effective for up to 1 year post-partum; however, its long-term effects are unknown. Group PFMT, given by a physiotherapist, has been proven to be as equally effective as individual therapy. Motherfit is a group-PFMT therapy with an emphasis on pelvic floor exercises, adherence and general fitness. Care-as-usual (CAU), if guideline driven, should, as first treatment option, consist of PFMT. Cost-effective strategies are of relevance, given the rise of health care costs. Motherfit group therapy has the potential to be cost-effective in women with urinary incontinence. Therefore, the objectives of the two current studies are: (1) to investigate whether intensive, supervised, pre-partum (MOTHERFIT1) or post-partum (MOTHERFIT2) pelvic-floor-muscle group therapy reduces 18-month post-partum severity of SUI compared to CAU and (2) whether MOTHERFIT1 OR MOTHERFIT 2 is more (cost-)effective compared to CAU.
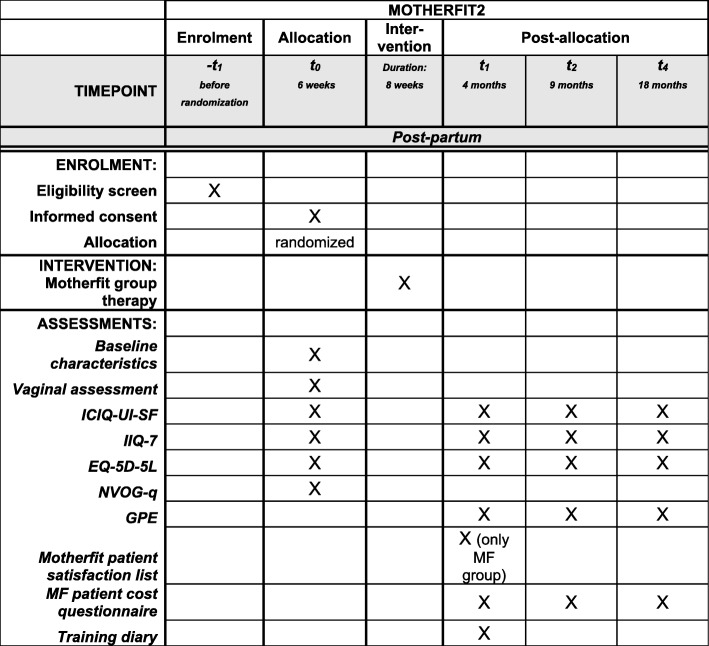
Methods: Two multi-centred, randomised controlled trials (MOTHERFIT1, n = 150, MOTHERFIT2, n = 90) will be performed. Participants will be recruited by their midwife or gynaecologist during their routine check. Participants with SUI will receive either motherfit group therapy or CAU. Motherfit group therapy consists of eight group sessions of 60 min each, instructed and supervised by a registered pelvic physiotherapist. Motherfit group therapy includes instructions on pelvic floor anatomy and how to contract, relax and train the pelvic-floor muscles correctly and is combined with general physical exercises. Adherence during and after motherfit will be stimulated by reinforcement techniques and a mobile app. The primary outcome measure is the absence of self-reported SUI based on the severity sum score of the International Consultation on Incontinence Questionnaire Short Form (ICIQ-UI-SF) at 18 months post-partum. Secondary outcomes evaluate quality of life, subjective improvement and health care costs.
Discussion: The motherfit studies are, to our knowledge, the first studies that evaluate both long-term results and health care costs compared to CAU in pregnant and post-partum women with SUI. If motherfit is shown to be (cost-)effective, implementation in peri-partum care should be considered.
Trial registration: Netherlands Trial Register, ID: NL5816 . Registered on 18 July 2016.
Keywords: Cost-effective; Group therapy; Motherfit; Pelvic-floor-muscle training; Peri-partum; Post-partum; Pre-partum; Pregnancy; Randomised controlled trial; Stress urinary incontinence.
Conflict of interest statement
Ethics approval and consent to participate
The studies MOTHERFIT1 and MOTHERFIT2 are registered as one trial in the Netherlands National Trial Register (NTR5971). The Medical Ethics Committee (METC) of the MUMC+ (central level) has approved MOTHERFIT1 at 21 December (METC162038) and MOTHERFIT2 at 22 December 2016 (METC162051). The remaining four participating hospitals (local level) received approval from their Medical Ethics Committees. Informed consent will be obtained from all study participants. This study has been designed in accordance with the Helsinki Accords and Dutch Medical Research Involving Human Subjects Act (WMO).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Cooper J, Annappa M, Quigley A, Dracocardos D, Bondili A, Mallen C. Prevalence of female urinary incontinence and its impact on quality of life in a cluster population in the United Kingdom (UK): a community survey. Prim Health Care Res Dev. 2015;16:377–382. doi: 10.1017/S1463423614000371. - DOI - PubMed
-
- Irwin DE, Milsom I, Hunskaar S, Reilly K, Kopp Z, Herschorn S, Coyne K, Kelleher C, Hampel C, Artibani W, Abrams P. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50:1306–1314. doi: 10.1016/j.eururo.2006.09.019. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
