

Health-related quality of life and prevalence of six chronic diseases in homeless and housed people: a cross-sectional study in London and Birmingham, England
- PMID: 31023754
- PMCID: PMC6501971
- DOI: 10.1136/bmjopen-2018-025192
Health-related quality of life and prevalence of six chronic diseases in homeless and housed people: a cross-sectional study in London and Birmingham, England
Abstract
Objectives: To compare health-related quality of life and prevalence of chronic diseases in housed and homeless populations.
Design: Cross-sectional survey with an age-matched and sex-matched housed comparison group.
Setting: Hostels, day centres and soup runs in London and Birmingham, England.
Participants: Homeless participants were either sleeping rough or living in hostels and had a history of sleeping rough. The comparison group was drawn from the Health Survey for England. The study included 1336 homeless and 13 360 housed participants.
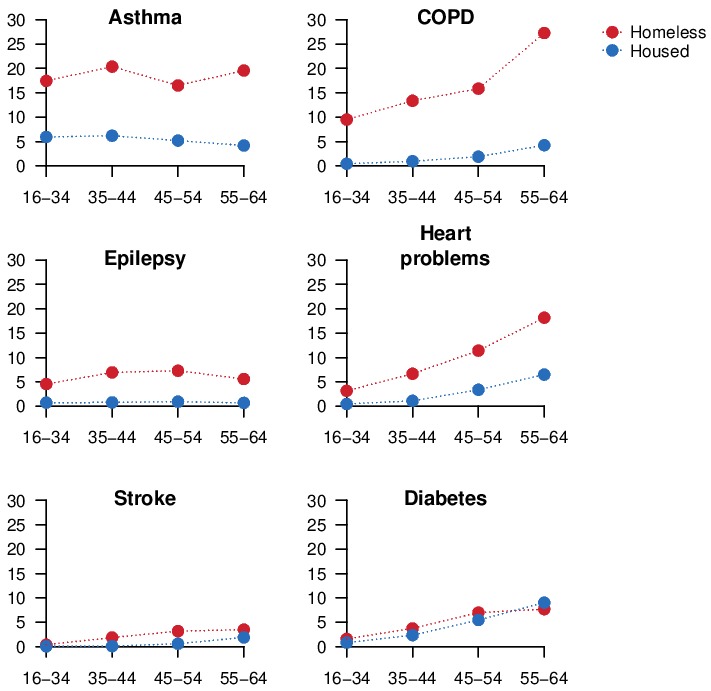
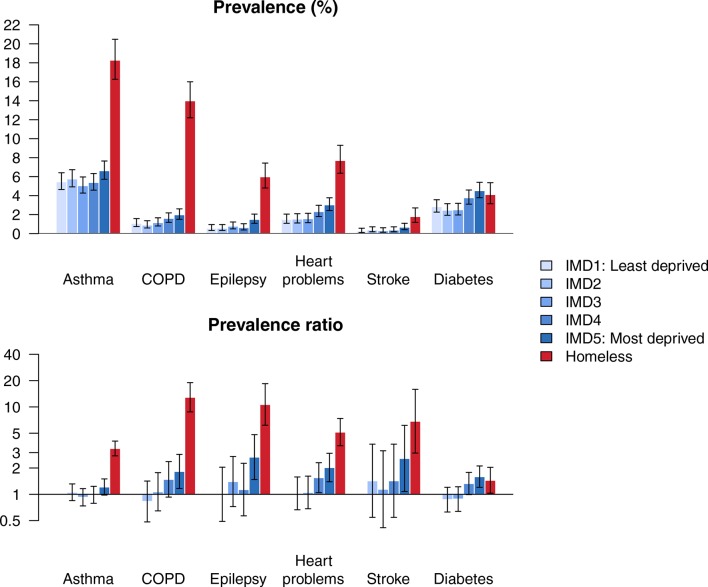
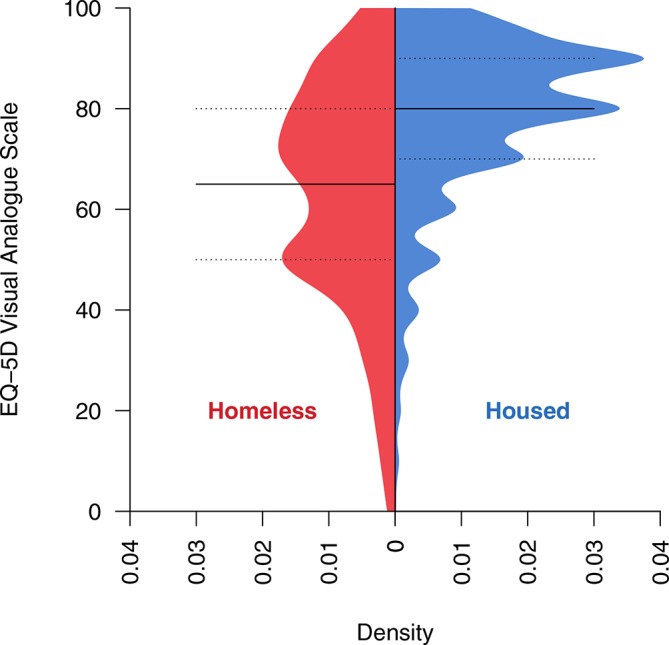
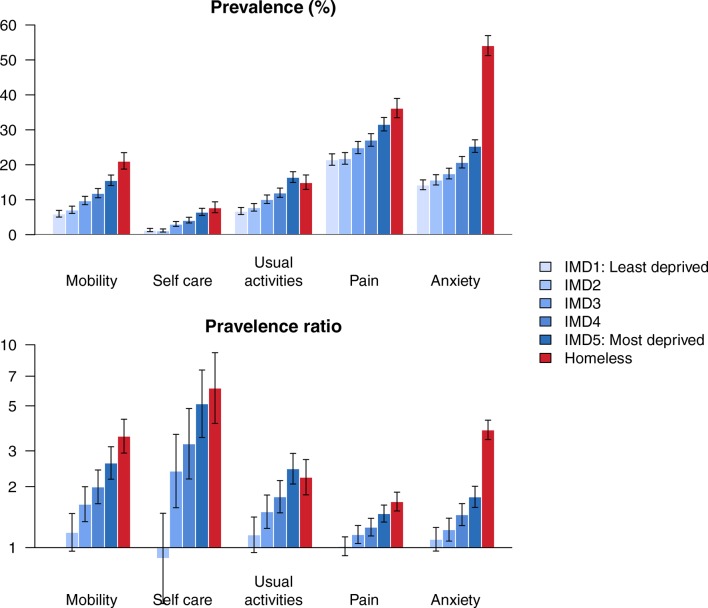
Outcome measures: Chronic diseases were self-reported asthma, chronic obstructive pulmonary disease (COPD), epilepsy, heart problems, stroke and diabetes. Health-related quality of life was measured using EQ-5D-3L.
Results: Housed participants in more deprived neighbourhoods were more likely to report disease. Homeless participants were substantially more likely than housed participants in the most deprived quintile to report all diseases except diabetes (which had similar prevalence in homeless participants and the most deprived housed group). For example, the prevalence of chronic obstructive pulmonary disease was 1.1% (95% CI 0.7% to 1.6%) in the least deprived housed quintile; 2.0% (95% CI 1.5% to 2.6%) in the most deprived housed quintile; and 14.0% (95% CI 12.2% to 16.0%) in the homeless group. Social gradients were also seen for problems in each EQ-5D-3L domain in the housed population, but homeless participants had similar likelihood of reporting problems as the most deprived housed group. The exception was problems related to anxiety, which were substantially more common in homeless people than any of the housed groups.
Conclusions: While differences in health between housed socioeconomic groups can be described as a 'slope', differences in health between housed and homeless people are better understood as a 'cliff'.
Keywords: epidemiology; homelessness; inequality; public health.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: AH is Trustee of the UK-based charity ’Pathway (healthcare for homeless people)'. AS is Clinical Lead for the Find & Treat Service; data were collected from homeless clients of this service.
Figures
References
-
- Ministry of Housing, Communities & Local Government. Rough Sleeping Statistics Autumn 2017, England (Revised). 2017. https://assets.publishing.service.gov.uk/government/uploads/system/uploa...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical