

Low-Dose Tacrolimus Prevents Dysregulated Peri-Conceptional Ovarian and Systemic Immune Cellular Homeostasis in Subjects with PCOS
- PMID: 31024070
- PMCID: PMC6484102
- DOI: 10.1038/s41598-019-42960-x
Low-Dose Tacrolimus Prevents Dysregulated Peri-Conceptional Ovarian and Systemic Immune Cellular Homeostasis in Subjects with PCOS
Abstract
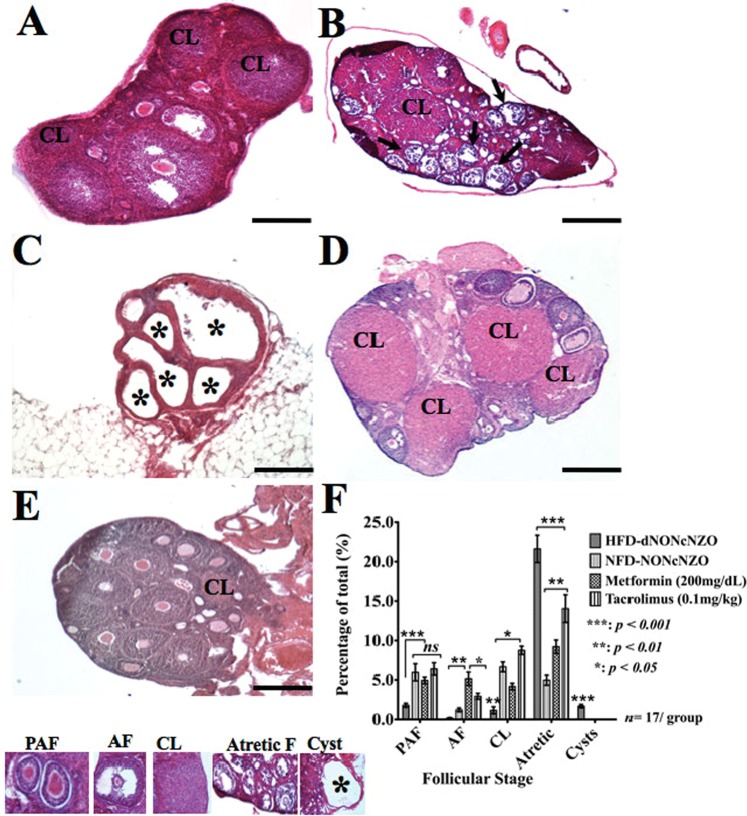
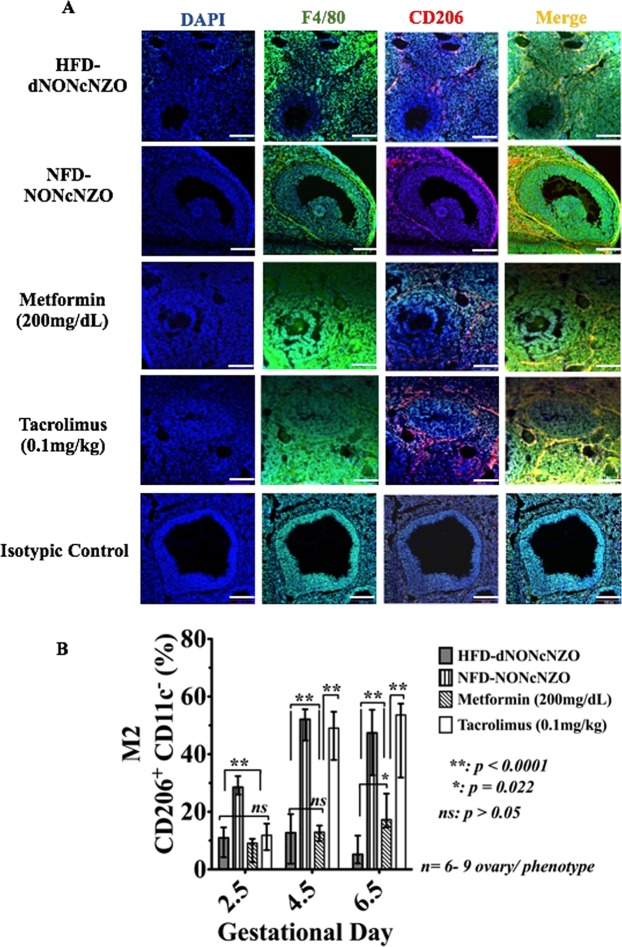
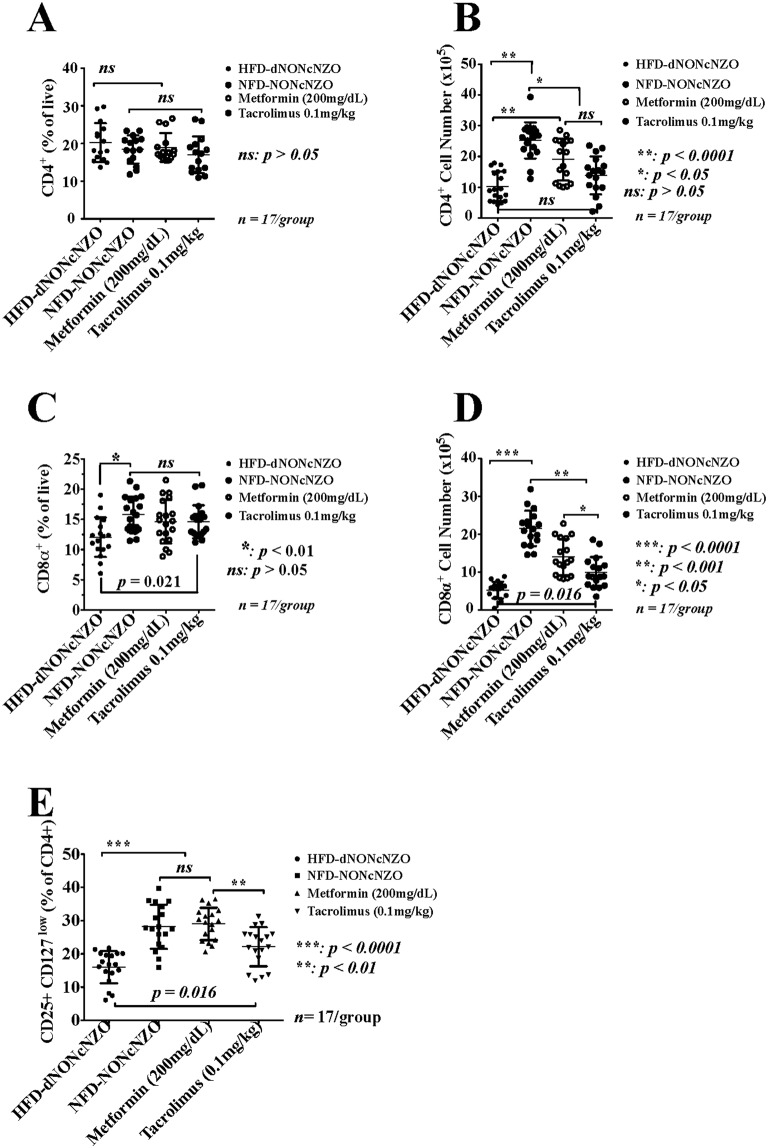
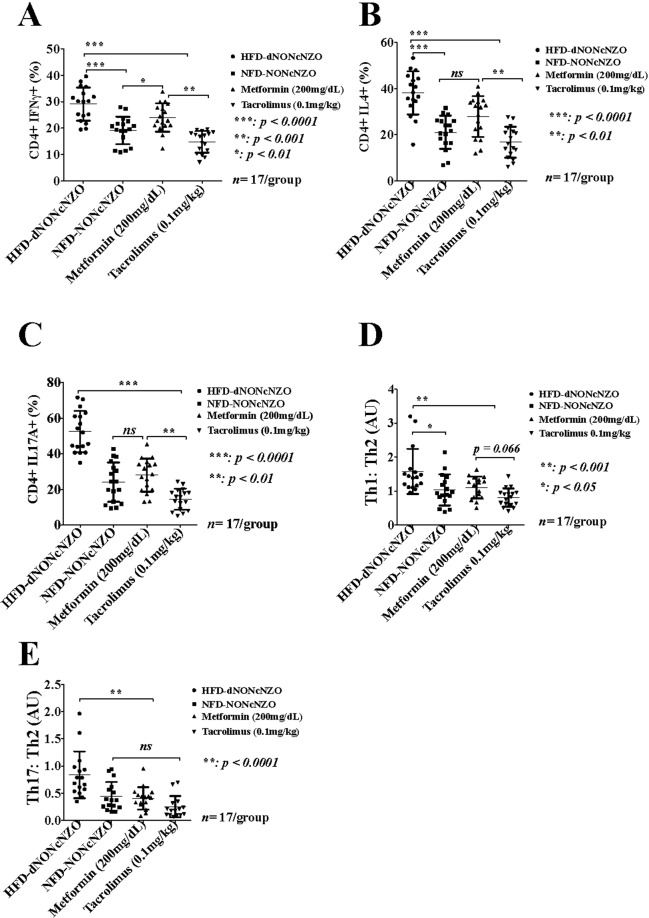
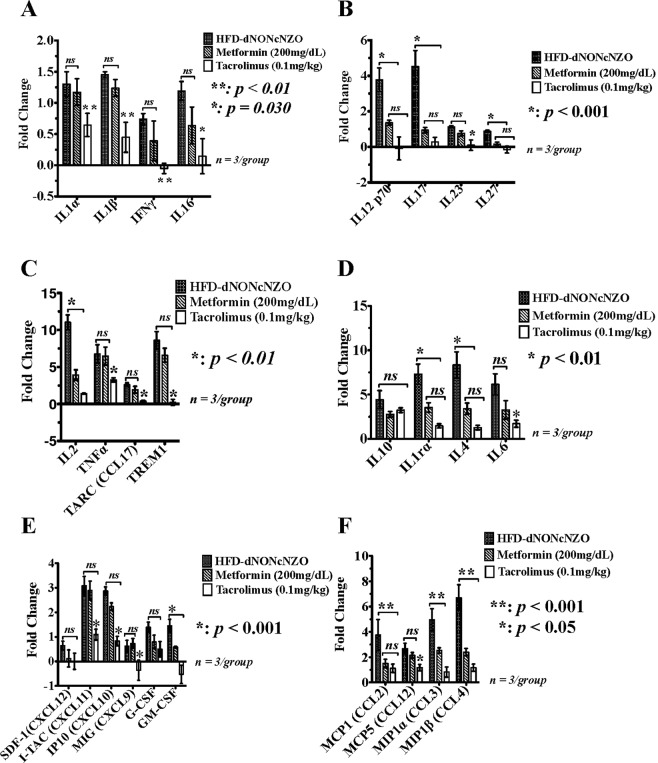
Polycystic ovary syndrome (PCOS) is characterized by failure of ovulation and is associated with obesity and chronic inflammation. Recent evidence suggests that anomalous activation of ovarian macrophages and numerical and functional deficits in the Th17 (CD4+IL17A+) and the CD4+CD25+CD127low Tregs plays crucial role in PCOS. We have shown that the pre-pregnancy use of tacrolimus prevents adverse reproductive outcomes in a mouse model of PCOS. Here we used the HFD-NONcNZO mice to test a hypothesized beneficial use of tacrolimus relative to metformin in favorably influencing the ovarian and systemic immune milieux conducive to gestational success in subjects with PCOS. Compared to normative controls, our data revealed an aberrant peri-conceptional suppression of the CD4+CD25+CD127low Tregs together with an overexpression of the Th17 T cells and lack of coordinated activation of ovarian macrophages in untreated HFD-dNONcNZO mice. Significant variances in treatment outcomes favoured the use of tacrolimus over metformin in treated mice. Consistent with the human fertility studies, this investigation reveals a beneficial systemic use of tacrolimus (0.1 mg/kg) in promoting early pregnancy in individuals with PCOS and suggests the need for further research into the selective inhibition of IL17A as a plausibly alternative immunotherapeutic approach in the clinical management of infertile individuals with PCOS.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
