

Cancer overdiagnosis: a biological challenge and clinical dilemma
- PMID: 31024081
- PMCID: PMC8819710
- DOI: 10.1038/s41568-019-0142-8
Cancer overdiagnosis: a biological challenge and clinical dilemma
Abstract
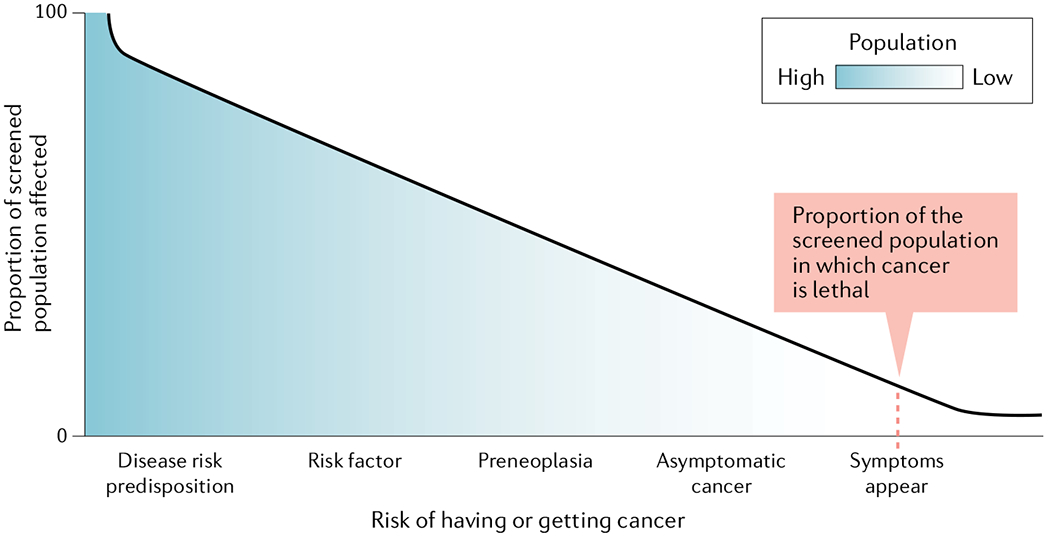
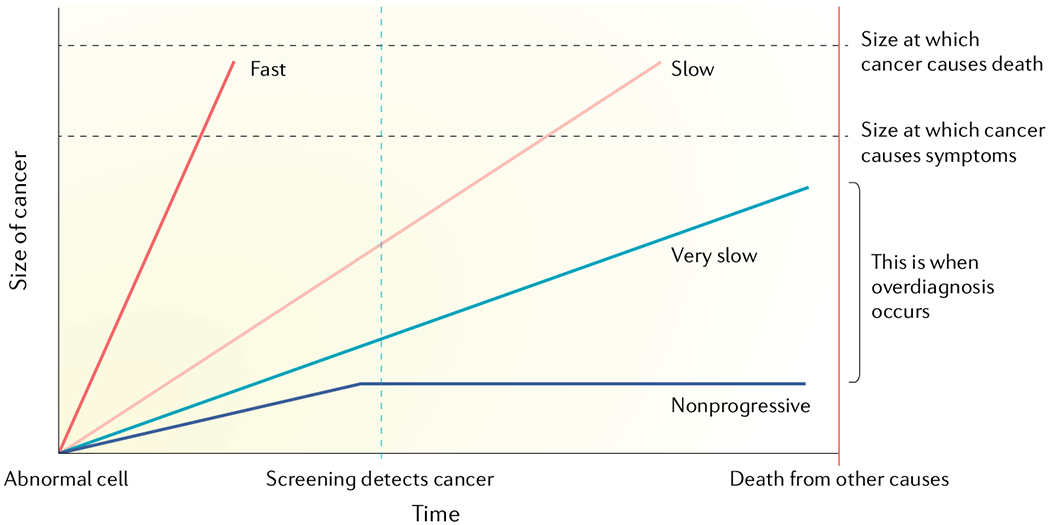
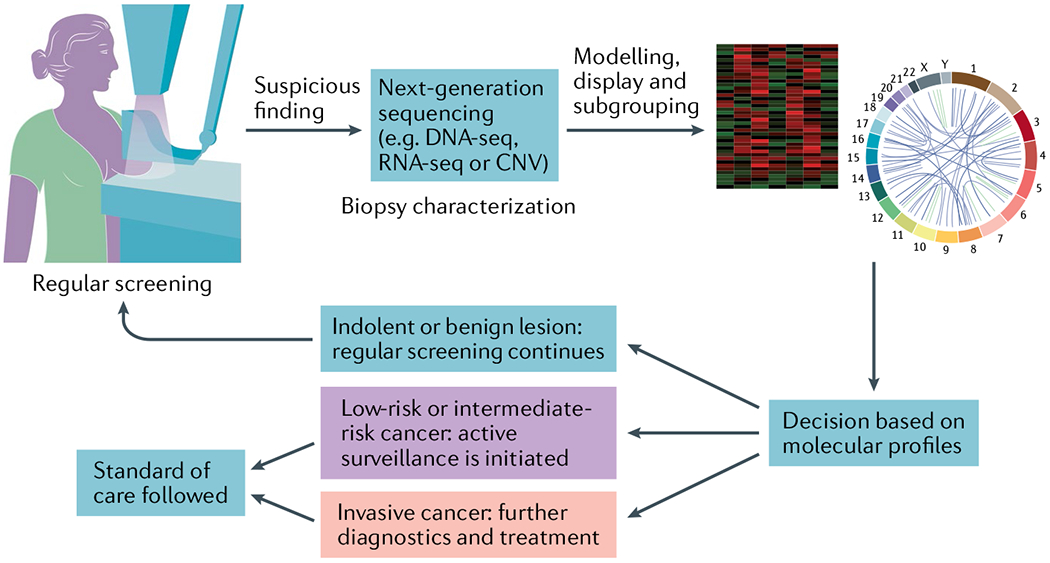
For cancer screening to be successful, it should primarily detect cancers with lethal potential or their precursors early, leading to therapy that reduces mortality and morbidity. Screening programmes have been successful for colon and cervical cancers, where subsequent surgical removal of precursor lesions has resulted in a reduction in cancer incidence and mortality. However, many types of cancer exhibit a range of heterogeneous behaviours and variable likelihoods of progression and death. Consequently, screening for some cancers may have minimal impact on mortality and may do more harm than good. Since the implementation of screening tests for certain cancers (for example, breast and prostate cancers), a spike in incidence of in situ and early-stage cancers has been observed, but a link to reduction in cancer-specific mortality has not been as clear. It is difficult to determine how many of these mortality reductions are due to screening and how many are due to improved treatments of tumours. In cancers with lower incidence but high mortality (for example, pancreatic cancer), screening has focused on high-risk populations, but challenges similar to those for general population screening remain, particularly with regard to finding lesions with difficult-to-characterize malignant potential (for example, intraductal papillary mucinous neoplasms). More sensitive screening methods are detecting smaller and smaller lesions, but this has not been accompanied by a comparable reduction in the incidence of invasive cancers. In this Opinion article, we focus on the contribution of screening in general and high-risk populations to overdiagnosis, the effects of overdiagnosis on patients and emerging strategies to reduce overdiagnosis of indolent cancers through an understanding of tumour heterogeneity, the biology of how cancers evolve and progress, the molecular and cellular features of early neoplasia and the dynamics of the interactions of early lesions with their surrounding tissue microenvironment.
Conflict of interest statement
Competing interests
The authors declare no competing interests.
Figures
References
-
- Weinberg DS & Schoen RE In the clinic. Screening for colorectal cancer. Ann. Intern. Med 160, ITC5–1 (2014). - PubMed
-
- Atkin WS et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet 375, 1624–1633 (2010). - PubMed
-
- Cooper GS, Chak A & Koroukian S The polyp detection rate of colonoscopy: a national study of Medicare beneficiaries. Am. J. Med 118, 1413 (2005). - PubMed
