

Endotype-Phenotype Patterns in Meniere's Disease Based on Gadolinium-Enhanced MRI of the Vestibular Aqueduct
- PMID: 31024416
- PMCID: PMC6459933
- DOI: 10.3389/fneur.2019.00303
Endotype-Phenotype Patterns in Meniere's Disease Based on Gadolinium-Enhanced MRI of the Vestibular Aqueduct
Abstract
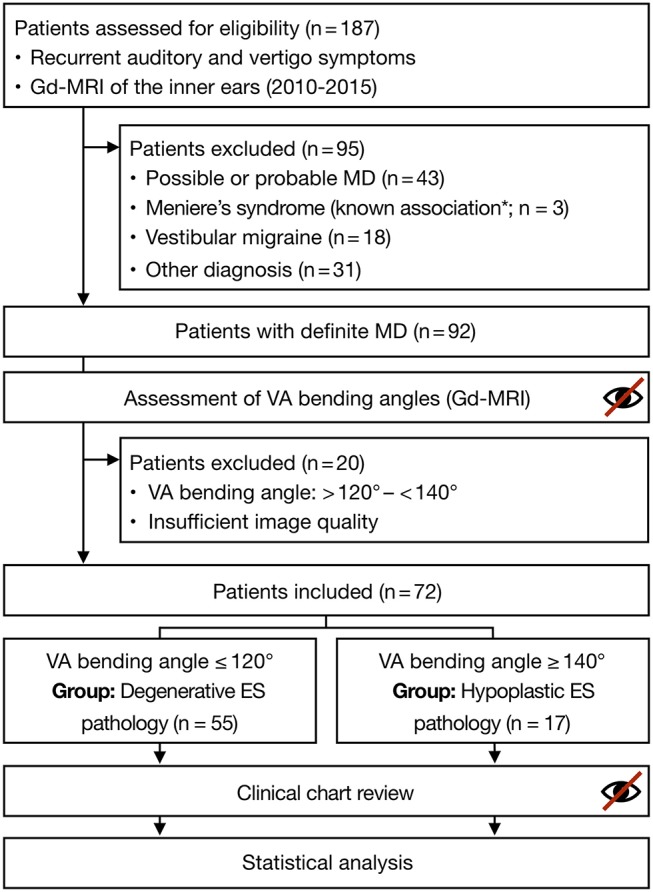
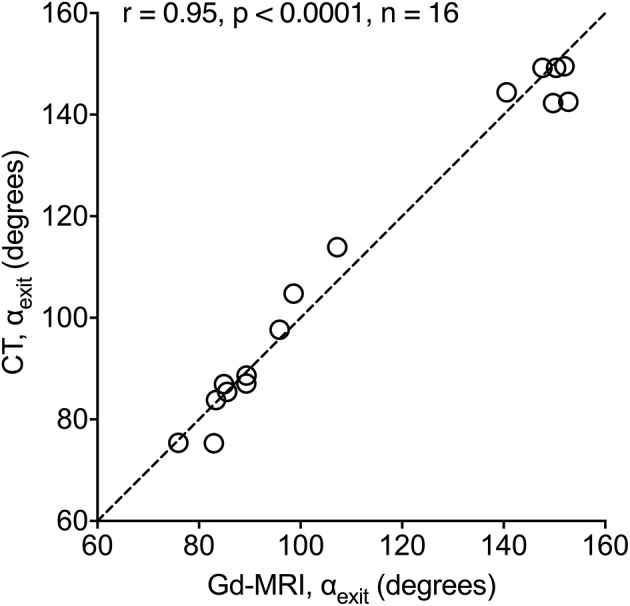
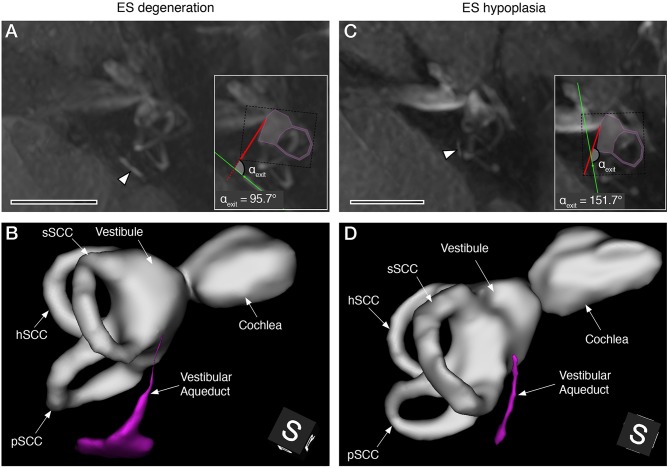
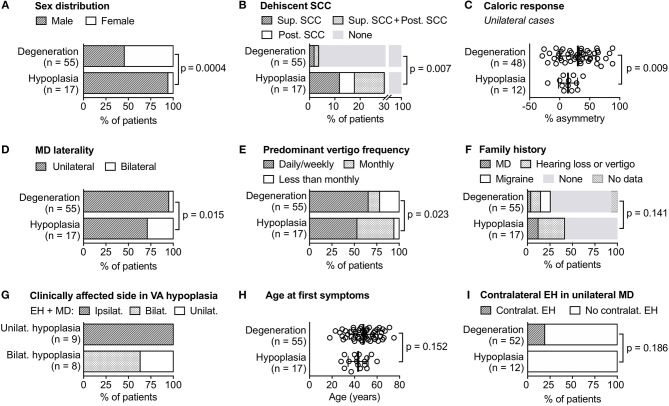
Two histopathological subtypes of Meniere's disease (MD) were recently described in a human post-mortem pathology study. The first subtype demonstrated a degenerating distal endolymphatic sac (ES) in the affected inner ear (subtype MD-dg); the second subtype (MD-hp) demonstrated an ES that was developmentally hypoplastic. The two subtypes were associated with different clinical disease features (phenotypes), suggesting that distinct endotype-phenotype patterns exist among MD patients. Therefore, clinical endotyping based on ES pathology may reveal clinically meaningful MD patient subgroups. Here, we retrospectively determined the ES pathologies of clinical MD patients (n = 72) who underwent intravenous delayed gadolinium-enhanced inner ear magnetic resonance imaging using previously established indirect radiographic markers for both ES pathologies. Phenotypic subgroup differences were evidenced; for example, the MD-dg group presented a higher average of vertigo attacks (ratio of vertigo patterns daily/weekly/other vs. monthly, MD-dg: 6.87: 1; MD-hp: 1.43: 1; p = 0.048) and more severely reduced vestibular function upon caloric testing (average caloric asymmetry ratio, MD-dg: 30.2% ± 30.4%; MD-hp: 13.5% ± 15.2%; p = 0.009), while the MD-hp group presented a predominantly male sex ratio (MD-hp: 0.06:1 [f/m]; MD-dg: 1.2:1 [f/m]; p = 0.0004), higher frequencies of bilateral clinical affection (MD-hp: 29.4%; MD-dg: 5.5%; p = 0.015), a positive family history for hearing loss/vertigo/MD (MD-hp: 41.2%; MD-dg: 15.7%; p = 0.028), and radiographic signs of concomitant temporal bone abnormalities, i.e., semicircular canal dehiscence (MD-hp: 29.4%; MD-dg: 3.6%; p = 0.007). In conclusion, this new endotyping approach may potentially improve the diagnosis, prognosis and clinical decision-making for individual MD patients.
Keywords: degeneration; endolymphatic sac; hypoplasia; patient subgroups; phenotype.
Figures
References
-
- Friberg U, Stahle J, Svedberg A. The natural course of Meniere's disease. Acta Otolaryngol Suppl. (1984) 406:72–7. - PubMed
-
- Merchant SN, Rauch SD, Nadol JBJ, Nadol JB, Jr. Meniere's disease. Eur Arch Otorhinolaryngol. (1995) 252:63–75. - PubMed
-
- Kitahara M. Bilateral aspects of meniere's disease: Meniere's disease with bilateral fluctuant hearing loss. Acta Otolaryngol. (1991) 485:74–7. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous