

A Computed Tomography-Based Radiomic Prognostic Marker of Advanced High-Grade Serous Ovarian Cancer Recurrence: A Multicenter Study
- PMID: 31024855
- PMCID: PMC6465630
- DOI: 10.3389/fonc.2019.00255
A Computed Tomography-Based Radiomic Prognostic Marker of Advanced High-Grade Serous Ovarian Cancer Recurrence: A Multicenter Study
Abstract
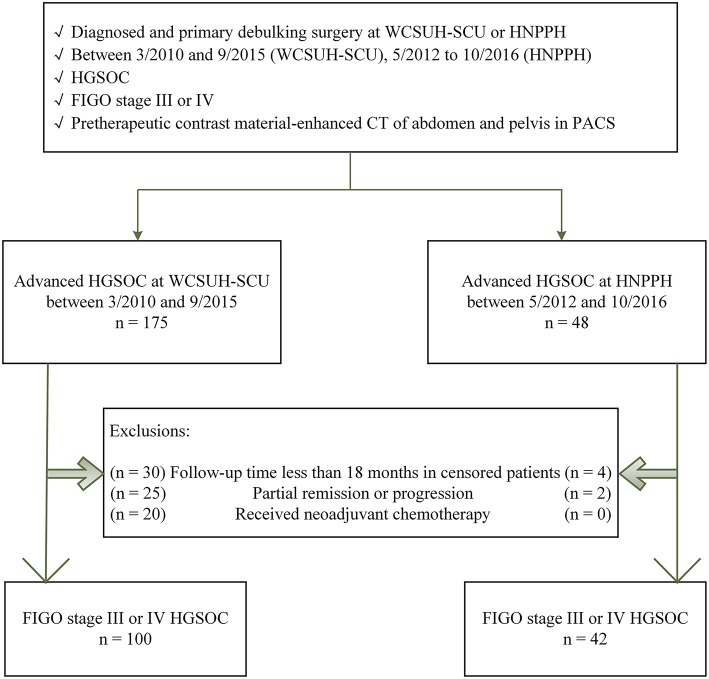
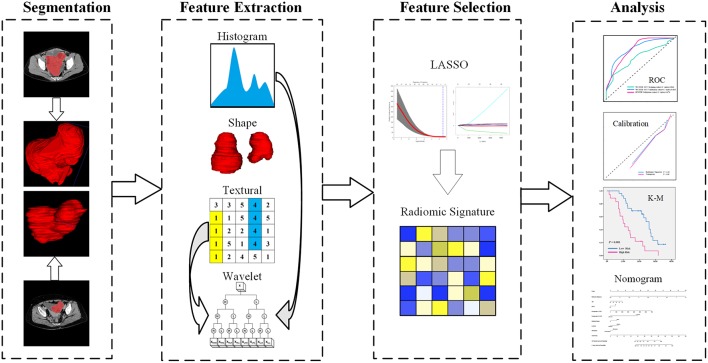
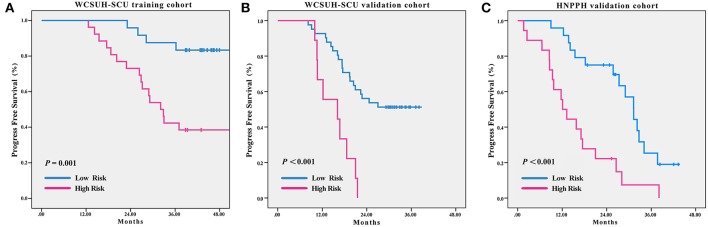
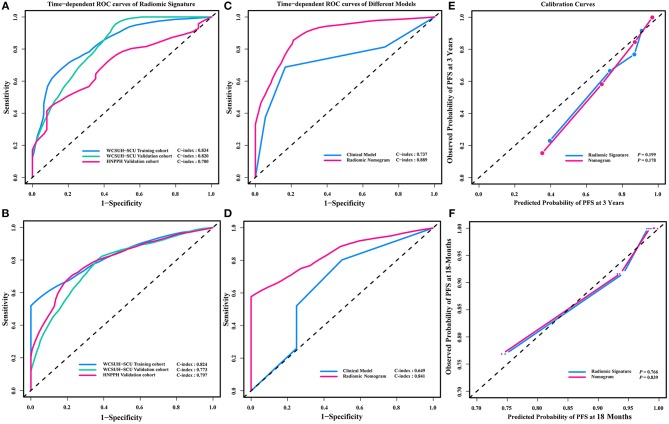
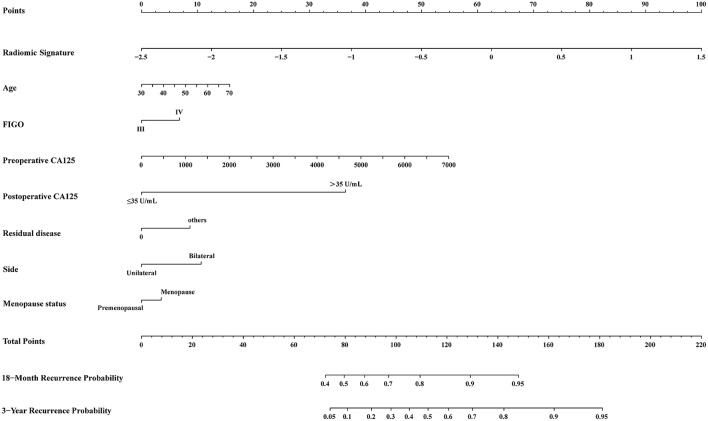
Objectives: We used radiomic analysis to establish a radiomic signature based on preoperative contrast enhanced computed tomography (CT) and explore its effectiveness as a novel recurrence risk prognostic marker for advanced high-grade serous ovarian cancer (HGSOC). Methods: This study had a retrospective multicenter (two hospitals in China) design and a radiomic analysis was performed using contrast enhanced CT in advanced HGSOC (FIGO stage III or IV) patients. We used a minimum 18-month follow-up period for all patients (median 38.8 months, range 18.8-81.8 months). All patients were divided into three cohorts according to the timing of their surgery and hospital stay: training cohort (TC) and internal validation cohort (IVC) were from one hospital, and independent external validation cohort (IEVC) was from another hospital. A total of 620 3-D radiomic features were extracted and a Lasso-Cox regression was used for feature dimension reduction and determination of radiomic signature. Finally, we combined the radiomic signature with seven common clinical variables to develop a novel nomogram using a multivariable Cox proportional hazards model. Results: A final 142 advanced HGSOC patients were enrolled. Patients were successfully divided into two groups with statistically significant differences based on radiomic signature, consisting of four radiomic features (log-rank test P = 0.001, <0.001, <0.001 for TC, IVC, and IEVC, respectively). The discrimination accuracies of radiomic signature for predicting recurrence risk within 18 months were 82.4% (95% CI, 77.8-87.0%), 77.3% (95% CI, 74.4-80.2%), and 79.7% (95% CI, 73.8-85.6%) for TC, IVC, and IEVC, respectively. Further, the discrimination accuracies of radiomic signature for predicting recurrence risk within 3 years were 83.4% (95% CI, 77.3-89.6%), 82.0% (95% CI, 78.9-85.1%), and 70.0% (95% CI, 63.6-76.4%) for TC, IVC, and IEVC, respectively. Finally, the accuracy of radiomic nomogram for predicting 18-month and 3-year recurrence risks were 84.1% (95% CI, 80.5-87.7%) and 88.9% (95% CI, 85.8-92.5%), respectively. Conclusions: Radiomic signature and radiomic nomogram may be low-cost, non-invasive means for successfully predicting risk for postoperative advanced HGSOC recurrence before or during the perioperative period. Radiomic signature is a potential prognostic marker that may allow for individualized evaluation of patients with advanced HGSOC.
Keywords: CT; advanced high-grade serous ovarian cancer; prognosis; radiomics; recurrence.
Figures
References
-
- Oza AM, Cook AD, Pfisterer J, Embleton A, Ledermann JA, Pujade-Lauraine E, et al. . Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol. (2015) 16:928–36. 10.1016/S1470-2045(15)00086-8 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources