

Analgesic efficacy and pharmacokinetics of epidural oxycodone in pain management after gynaecological laparoscopy-A randomised, double blind, active control, double-dummy clinical comparison with intravenous administration
- PMID: 31026086
- PMCID: PMC6624386
- DOI: 10.1111/bcp.13971
Analgesic efficacy and pharmacokinetics of epidural oxycodone in pain management after gynaecological laparoscopy-A randomised, double blind, active control, double-dummy clinical comparison with intravenous administration
Abstract
Aims: Early pain after laparoscopy is often severe. Oxycodone is a feasible analgesic option after laparoscopy, but there are sparse data on epidural administration. The aim was to evaluate the analgesic efficacy and pharmacokinetics of a single dose of epidural oxycodone as a part of multimodal analgesia after gynaecological laparoscopy.
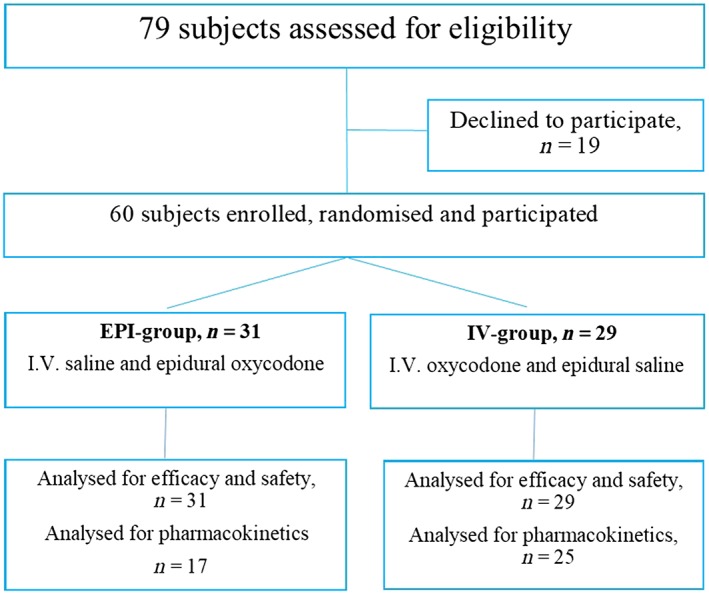
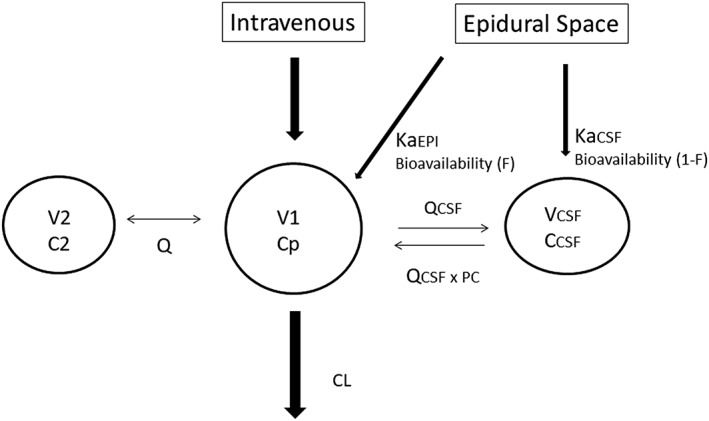
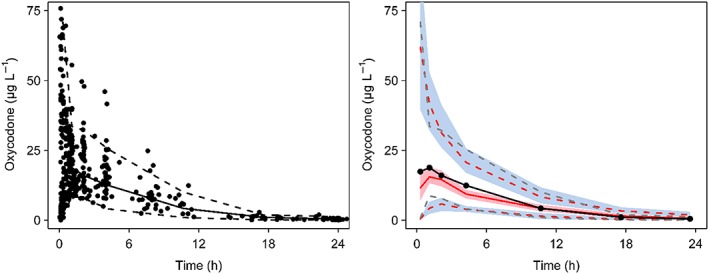
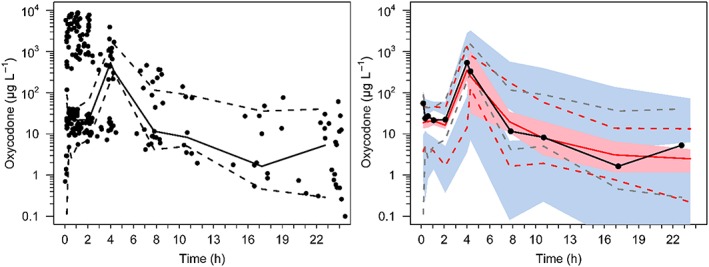
Methods: Women (n = 60), aged 23-71 years, undergoing elective gynaecological laparoscopy, were administrated either epidural oxycodone 0.1 mg kg-1 and intravenous (i.v.) saline (EPI-group n = 31), or epidural saline and i.v. oxycodone 0.1 mg kg-1 (IV-group = 29) in a randomised, double blind, active control, double dummy clinical trial. A pharmacokinetic model was developed using population modelling of plasma and cerebrospinal fluid (CSF) concentrations obtained in these patients and data of 2 published studies. The primary outcome was the amount of i.v. fentanyl for rescue analgesia during the first 4 hours.
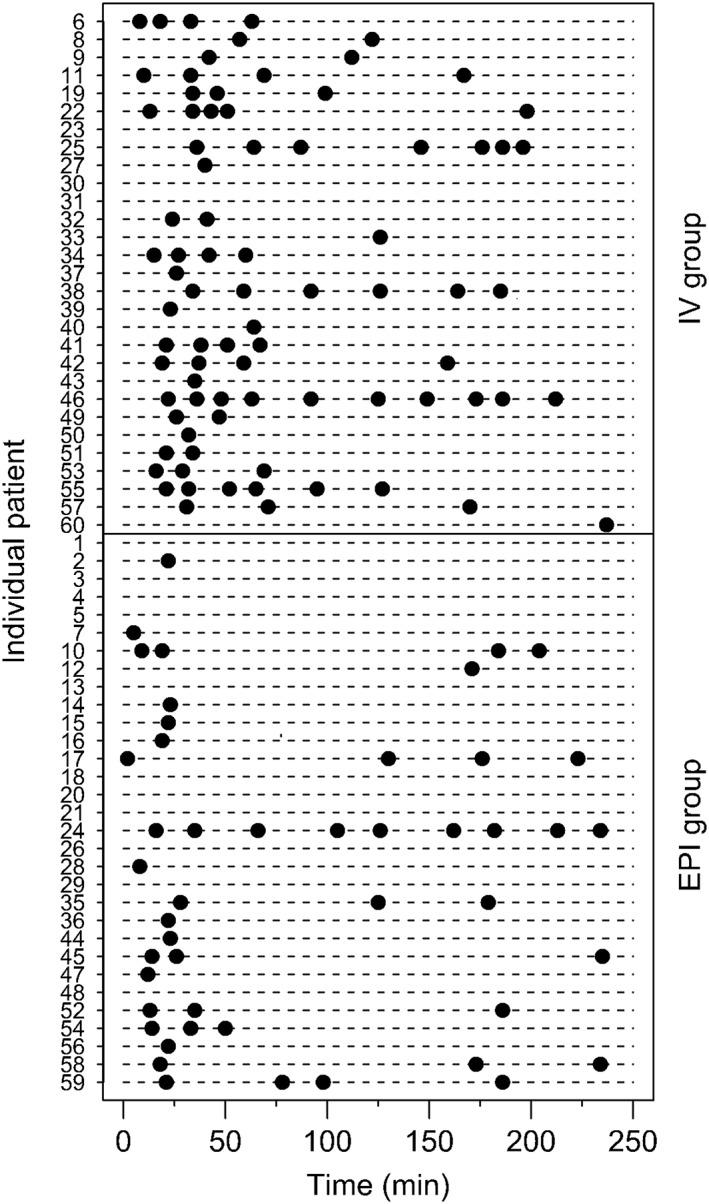
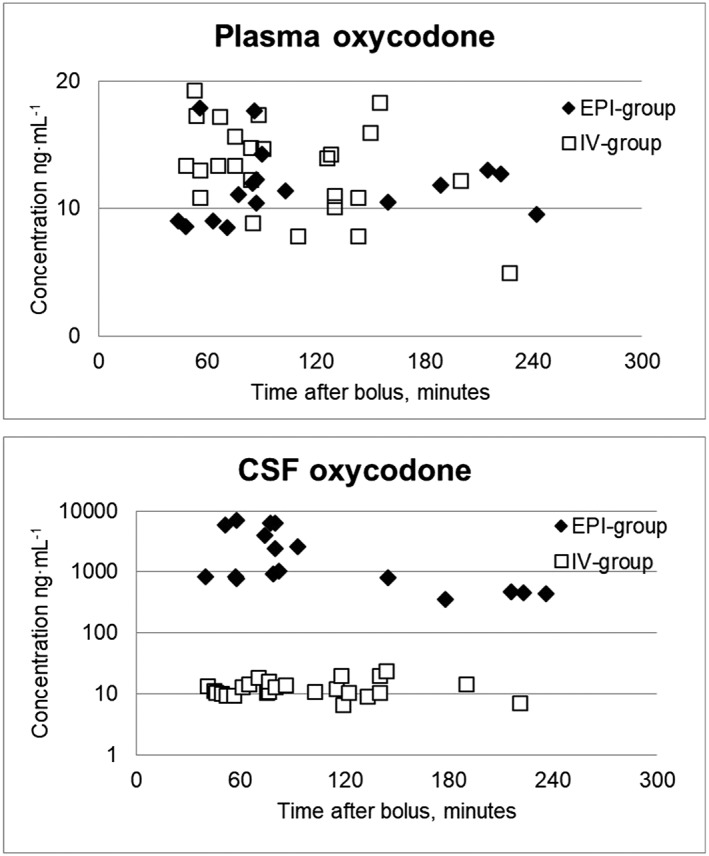
Results: Twenty of the 31 patients in the EPI-group and 26 of the 29 patients in the IV-group needed i.v. fentanyl for rescue analgesia, P = .021. The median (interquartile range) number of fentanyl doses were 1.0 (1.0-3.0) in the EPI-group and 2.5 (1.0-4.0) doses in the IV-group, P = .008. Plasma concentrations were similar, but CSF concentrations were 100-fold higher in the EPI-group. The population model indicated that 60% of oxycodone injected into the epidural space enters into CSF and 40% is absorbed into the systemic circulation.
Conclusions: The data support superiority of epidural administration of oxycodone compared to i.v. administration during the first hours after laparoscopic surgery. This is likely to be based on enhanced permeation into the central nervous system after epidural administration.
Keywords: analgesia; epidural; oxycodone; pharmacokinetics.
© 2019 The British Pharmacological Society.
Conflict of interest statement
There are no competing interests to declare.
Figures
References
-
- Kokki M, Broms S, Eskelinen M, Rasanen I, Ojanperä I, Kokki H. Analgesic concentrations of oxycodone‐‐a prospective clinical PK/PD study in patients with laparoscopic cholecystectomy. Basic Clin Pharmacol Toxicol. 2012;110(5):469–475. - PubMed
-
- Sjövall S, Kokki M, Kokki H. Laparoscopic surgery: a narrative review of pharmacotherapy in pain management. Drugs. 2015;75(16):1867–1889. - PubMed
-
- Lenz H, Sandvik L, Qvigstad E, Bjerkelund CE, Raeder J. A comparison of intravenous oxycodone and intravenous morphine in patient‐controlled postoperative analgesia after laparoscopic hysterectomy. Anesth Analg. 2009;109(4):1279–1283. - PubMed
-
- Kalso E, Pöyhiä R, Onnela P, Linko K, Tigerstedt I, Tammisto T. Intravenous morphine and oxycodone for pain after abdominal surgery. Acta Anaesthesiol Scand. 1991;35(7):642–646. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
