

Deciphering the complex interplay between microbiota, HPV, inflammation and cancer through cervicovaginal metabolic profiling
- PMID: 31027917
- PMCID: PMC6604110
- DOI: 10.1016/j.ebiom.2019.04.028
Deciphering the complex interplay between microbiota, HPV, inflammation and cancer through cervicovaginal metabolic profiling
Abstract
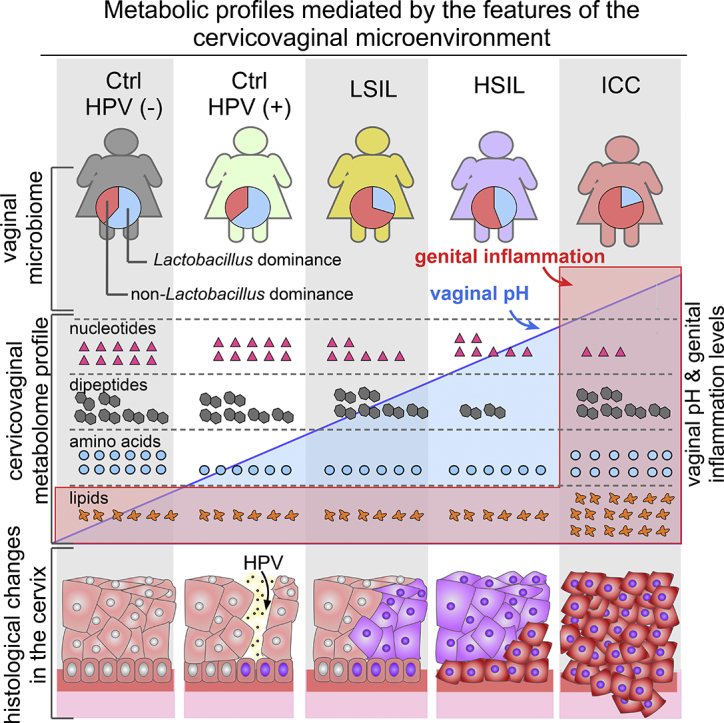
Background: Dysbiotic vaginal microbiota have been implicated as contributors to persistent HPV-mediated cervical carcinogenesis and genital inflammation with mechanisms unknown. Given that cancer is a metabolic disease, metabolic profiling of the cervicovaginal microenvironment has the potential to reveal the functional interplay between the host and microbes in HPV persistence and progression to cancer.
Methods: Our study design included HPV-negative/positive controls, women with low-grade and high-grade cervical dysplasia, or cervical cancer (n = 78). Metabolic fingerprints were profiled using liquid chromatography-mass spectrometry. Vaginal microbiota and genital inflammation were analysed using 16S rRNA gene sequencing and immunoassays, respectively. We used an integrative bioinformatic pipeline to reveal host and microbe contributions to the metabolome and to comprehensively assess the link between HPV, microbiota, inflammation and cervical disease.
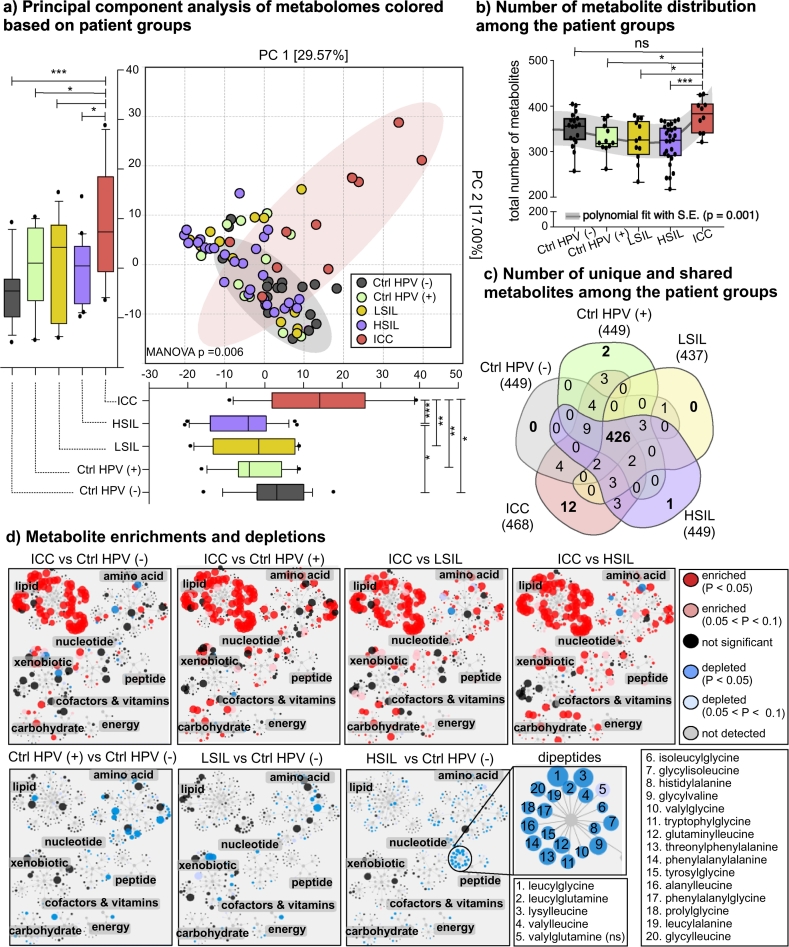
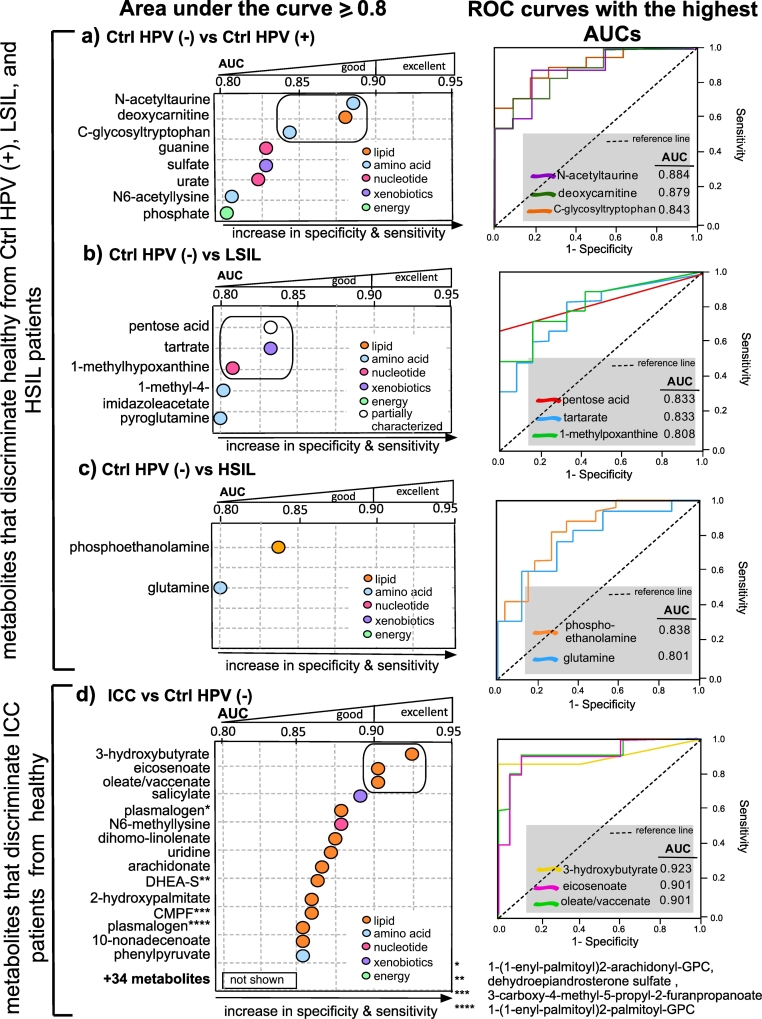
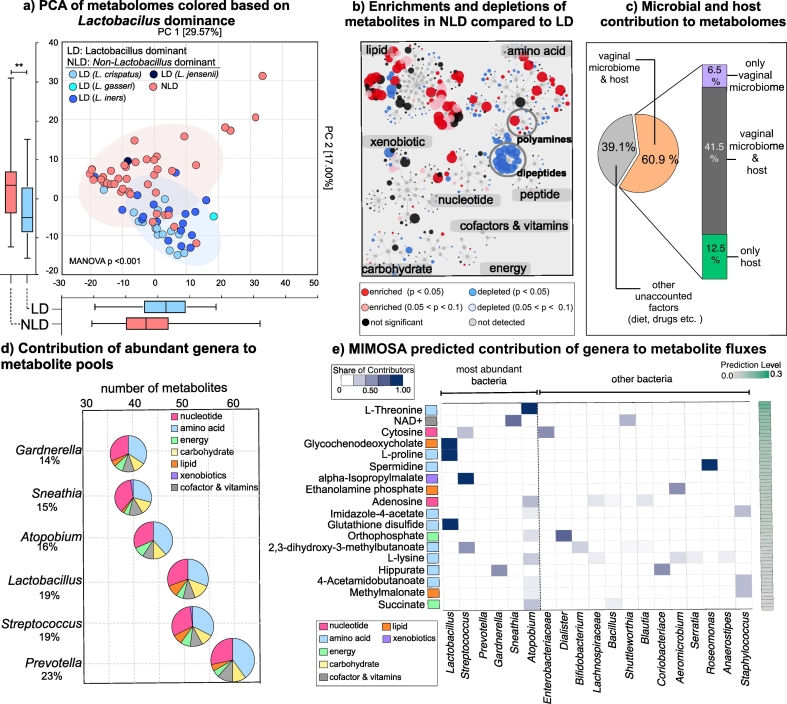
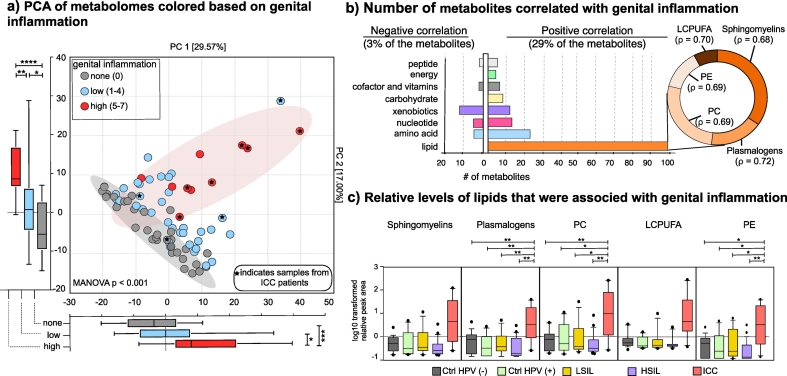
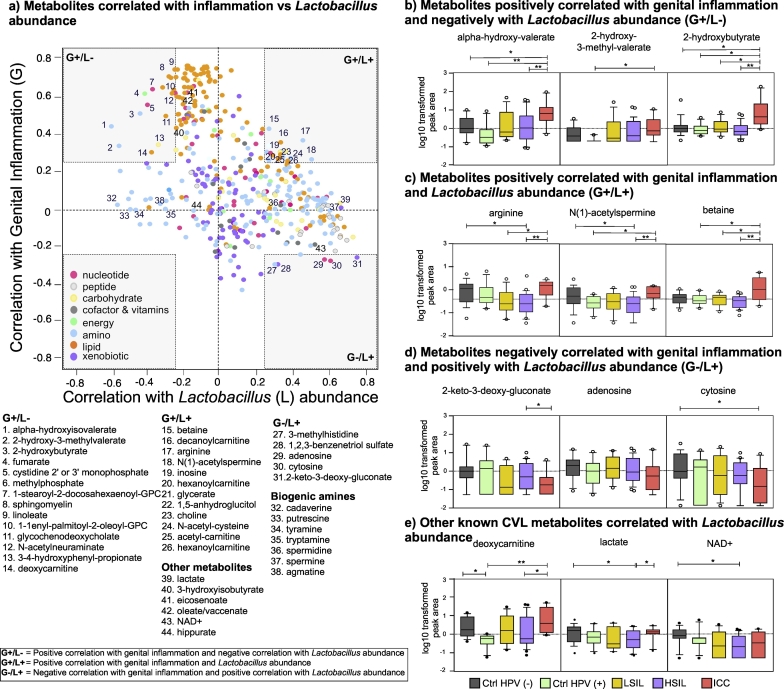
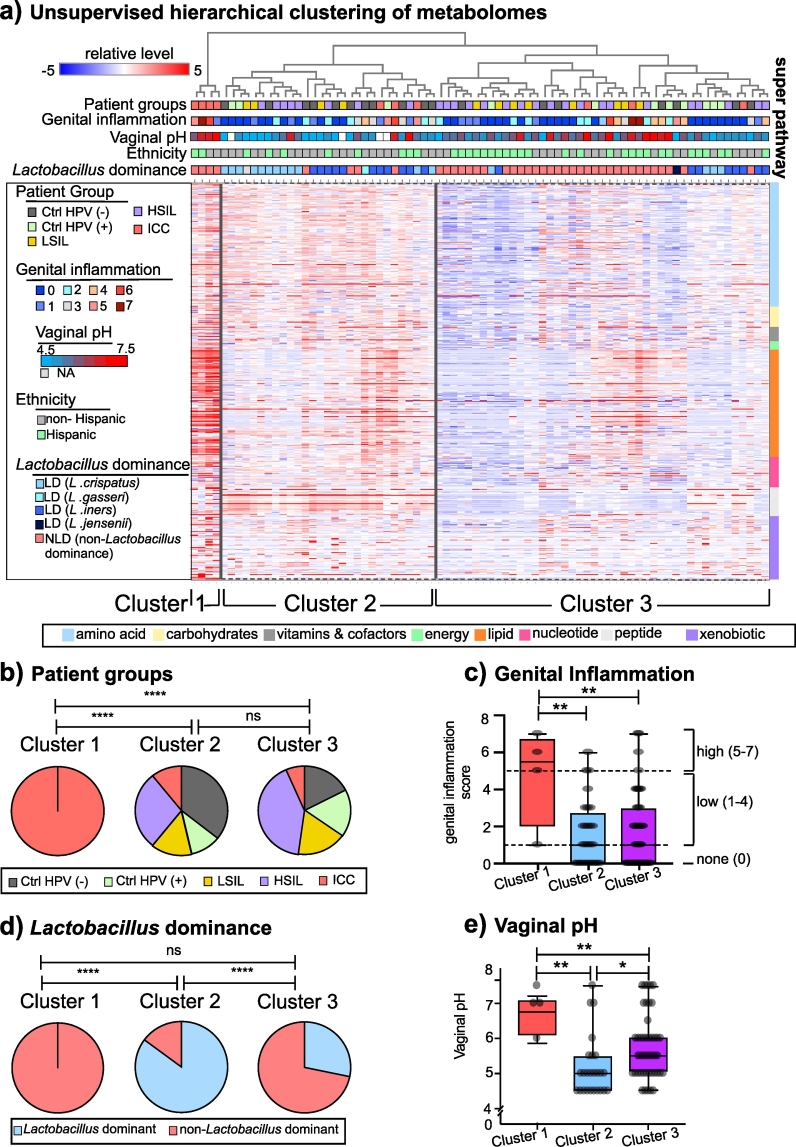
Findings: Metabolic analysis yielded 475 metabolites with known identities. Unique metabolic fingerprints discriminated patient groups from healthy controls. Three-hydroxybutyrate, eicosenoate, and oleate/vaccenate discriminated (with excellent capacity) between cancer patients versus the healthy participants. Sphingolipids, plasmalogens, and linoleate positively correlated with genital inflammation. Non-Lactobacillus dominant communities, particularly in high-grade dysplasia, perturbed amino acid and nucleotide metabolisms. Adenosine and cytosine correlated positively with Lactobacillus abundance and negatively with genital inflammation. Glycochenodeoxycholate and carnitine metabolisms connected non-Lactobacillus dominance to genital inflammation.
Interpretation: Cervicovaginal metabolic profiles were driven by cancer followed by genital inflammation, HPV infection, and vaginal microbiota. This study provides evidence for metabolite-driven complex host-microbe interactions as hallmarks of cervical cancer with future translational potential. FUND: Flinn Foundation (#1974), Banner Foundation Obstetrics/Gynecology, and NIH NCI (P30-CA023074).
Keywords: Amino acid degradation; Cervical dysplasia and cancer; Genital inflammation; Host-microbe interactions; Lactobacillus abundance; Lipids and nucleotides; Vaginal dysbiosis.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Schiffman M., Doorbar J., Wentzensen N., De Sanjosé S., Fakhry C., Monk B.J. Carcinogenic human papillomavirus infection. Nat Rev Dis Prim. 2016;2 - PubMed
-
- Bray F., Jacques F., Soerjomataram I., Siegel R., Torre L., Jemal A. Global Cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Carter J.R., Ding Z., Rose B.R. HPV infection and cervical disease: a review. Aust New Zeal J Obstet Gynaecol. 2011;51(2):103–108. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
