

Outcomes of direct lateral interbody fusion (DLIF) in an Australian cohort
- PMID: 31032433
- PMCID: PMC6465476
- DOI: 10.21037/jss.2019.01.08
Outcomes of direct lateral interbody fusion (DLIF) in an Australian cohort
Abstract
Background: Direct lateral interbody fusion (DLIF) mitigates many of the vascular complications and bony resections associated with other interbody fusion techniques. However, there are concerns regarding postoperative neural complications and that indirect decompression of the foramen has not been consistently demonstrated. This study prospectively assessed the clinical and radiological outcomes and the complication rates of the DLIF approach.
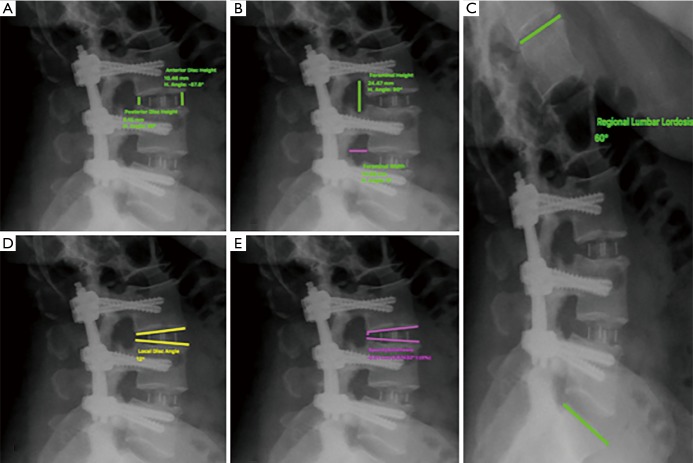
Methods: A prospective review was conducted of the first 50 consecutive DLIF cases of a single neurosurgeon between 2010 and 2014. Clinical outcomes were assessed using Visual Analogue Scale (VAS), Oswestry Disability Index (ODI) and Roland Morris Disability Questionnaire (RMDQ) surveys. Radiological outcomes, including spondylolisthesis, disc height, local disc angle, lumbar lordosis and foraminal height and width, were measured using Surgimap Spine software at the preoperative, 6 weeks, 6 months, and 12 months postoperative follow-up. Complication rates were also reported.
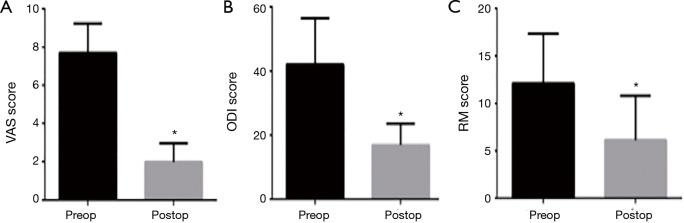
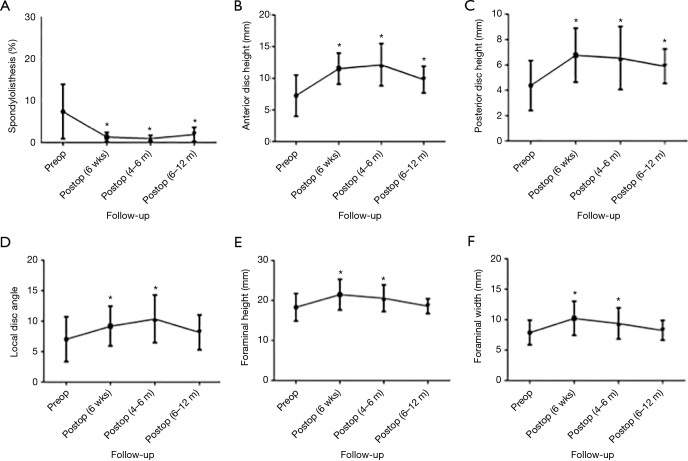
Results: A total of 50 patients (84 levels) were treated with DLIF. The mean patient age was 68.2±9.8 years and 62.0% were female. At latest follow-up, mean VAS pain score improved from 7.7±1.5 to 1.9±0.9 (P<0.0001), mean ODI improved from 42.1±14.5 to 16.9±6.7 (P<0.0001) and mean RMDQ score improved from 12.1±5.2 to 6.2±4.7 (P<0.0001). Mean spondylolisthesis reduced from 7.5%±6.5% to 1.3%±1.1% at 6 weeks (P<0.0001), 0.95%±0.74% at 6 months (P<0.0001) and recurred to 1.9%±1.7% at 12 months postoperatively (P=0.0006). Mean anterior disc height improved from 7.3±3.2 to 11.6±2.5 mm at 6 weeks (P<0.0001), 12.2±3.3 mm at 6 months (P<0.0001) and 9.8±2.1 mm at 12 months (P=0.0032) postoperatively. Mean posterior disc height improved from 4.4±2.0 to 6.8±2.1 mm at 6 weeks (P<0.0001), 6.6±2.5 mm at 6 months (P=0.0003), and 5.9±1.4 mm at 12 months (P=0.0039) postoperatively. Mean local disc angle improved from 7.0°±3.7° to 9.2°±3.3° at 6 weeks (P=0.0072), 10.4°±3.9° at 6 months (P=0.0013) and 8.2°±2.9° at 12 months (P=0.2487) postoperatively. No significant postoperative changes in lumbar lordosis were observed. Mean foraminal height improved from 18.3±3.5 to 21.5±3.9 mm at 6 weeks (P=0.0004), 20.6±3.4 mm at 6 months (P=0.0266), and 18.7±1.9 mm at 12 months (P=0.8021) postoperatively. Mean foraminal width improved from 7.9±2.0 to 10.2±2.8 mm at 6 weeks (P=0.0001), 9.4±2.6 mm at 6 months (P=0.0219) and 8.3±1.6 mm at 12 months (P=0.5734) postoperatively. Fusion rate at 6 and 12 months was 62.2% and 89.2%, respectively. A total of 6 patients (12%) had postoperative complications. Three patients (6%) had pain-related psoas muscle weakness and 3 patients (6%) had sensory neural complications that had resolved entirely by 8 and 16 weeks postoperatively, respectively.
Conclusions: The study provides encouraging short and medium-term clinical and radiological results for DLIF. In this patient series, there was a low complication rate with no permanent neural injury reported.
Keywords: Direct lateral interbody fusion (DLIF); clinical outcomes; lateral lumbar interbody fusion (LLIF); minimally invasive spine surgery; radiological outcomes.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Radiological and clinical outcomes following extreme lateral interbody fusion.J Neurosurg Spine. 2014 Jun;20(6):623-35. doi: 10.3171/2014.1.SPINE13569. Epub 2014 Apr 4. J Neurosurg Spine. 2014. PMID: 24702513
-
Short-term outcomes of lateral lumbar interbody fusion without decompression for the treatment of symptomatic degenerative spondylolisthesis at L4-5.Neurosurg Focus. 2018 Jan;44(1):E6. doi: 10.3171/2017.10.FOCUS17566. Neurosurg Focus. 2018. PMID: 29290128
-
Direct lateral lumbar interbody fusion: clinical and radiological outcomes.J Korean Neurosurg Soc. 2014 May;55(5):248-54. doi: 10.3340/jkns.2014.55.5.248. Epub 2014 May 31. J Korean Neurosurg Soc. 2014. PMID: 25132930 Free PMC article.
-
Lateral Lumbar Interbody Fusion: What Is the Evidence of Indirect Neural Decompression? A Systematic Review of the Literature.HSS J. 2020 Jul;16(2):143-154. doi: 10.1007/s11420-019-09734-7. Epub 2020 Mar 20. HSS J. 2020. PMID: 32523482 Free PMC article. Review.
-
Efficacy and Safety of the Extreme Lateral Interbody Fusion (XLIF) Technique in Spine Surgery: Meta-Analysis of 1409 Patients.J Clin Med. 2024 Feb 7;13(4):960. doi: 10.3390/jcm13040960. J Clin Med. 2024. PMID: 38398273 Free PMC article. Review.
Cited by
-
L4/5 accessibility for extreme lateral interbody fusion (XLIF): a radiological study.J Orthop Surg Res. 2022 Nov 11;17(1):483. doi: 10.1186/s13018-022-03320-0. J Orthop Surg Res. 2022. PMID: 36369101 Free PMC article.
-
Restoring spinopelvic harmony with lateral lumbar interbody fusion: is it a realistic goal?J Spine Surg. 2020 Dec;6(4):639-649. doi: 10.21037/jss-20-605. J Spine Surg. 2020. PMID: 33447666 Free PMC article.
-
Indirect decompression via oblique lumbar interbody fusion is sufficient for treatment of lumbar foraminal stenosis.Front Surg. 2022 Aug 18;9:911514. doi: 10.3389/fsurg.2022.911514. eCollection 2022. Front Surg. 2022. PMID: 36061052 Free PMC article.
-
Changes in Segmental and Lumbar Lordosis After Lateral Lumbar Interbody Fusion With Different Lordotic Cage Angulations.Int J Spine Surg. 2021 Jun;15(3):440-448. doi: 10.14444/8066. Epub 2021 May 7. Int J Spine Surg. 2021. PMID: 33963028 Free PMC article.
-
iSurgARy: A mobile augmented reality solution for ventriculostomy in resource-limited settings.Healthc Technol Lett. 2025 Jan 15;12(1):e12118. doi: 10.1049/htl2.12118. eCollection 2025 Jan-Dec. Healthc Technol Lett. 2025. PMID: 39816703 Free PMC article.
References
LinkOut - more resources
Full Text Sources