

Adult intradural intramedullary astrocytomas: a multicenter analysis
- PMID: 31032435
- PMCID: PMC6465470
- DOI: 10.21037/jss.2018.12.06
Adult intradural intramedullary astrocytomas: a multicenter analysis
Abstract
Background: Intramedullary tumors constitute approximately 20-30% of all spinal cord tumors and approximately 30-40% of these are astrocytomas. Furthermore, they comprise only about 2-4% of all primary central nervous system (CNS) tumors. Due to their rarity and poor prognosis, large population-based studies are needed to assess the epidemiology and survival risk factors associated with these tumors in the hope of improving outcomes. The authors undertook this retrospective study to explore factors that may influence survival in adult patients with intramedullary astrocytomas.
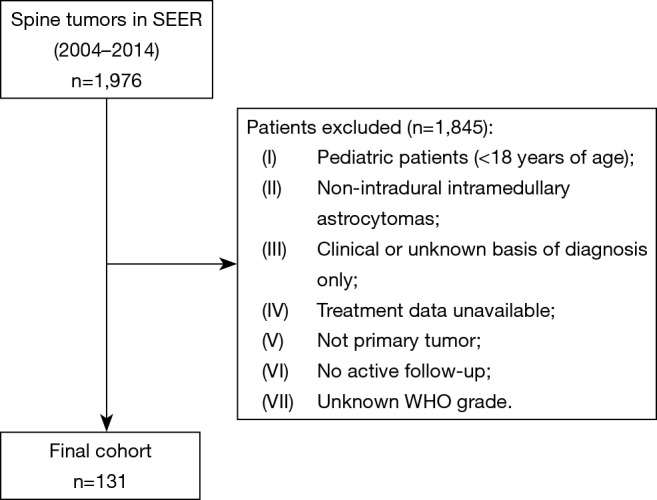
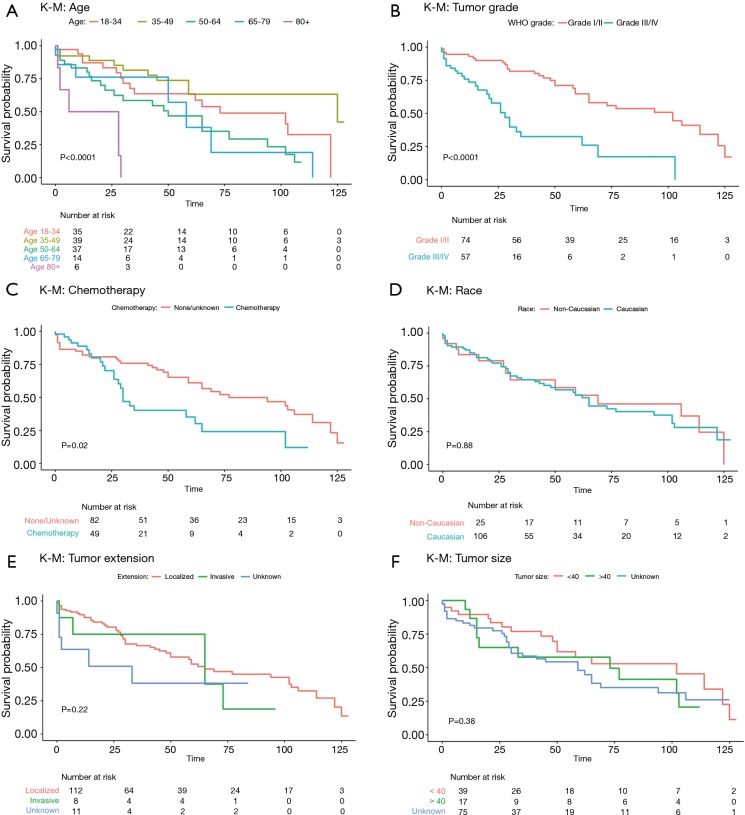
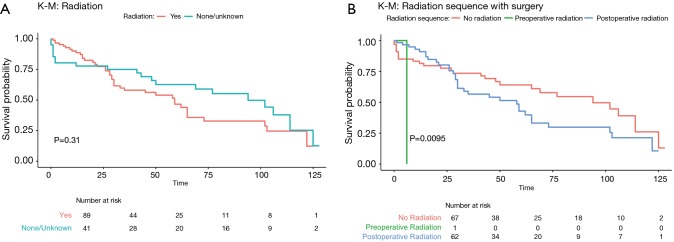
Methods: Utilizing the Surveillance, Epidemiology, and End Results (SEER) database, a prospective cancer registry, the authors retrospectively assessed survival in histologically confirmed, intramedullary spinal cord astrocytomas in patients 18 years of age and older. Survival was described with Kaplan-Meier curves and multivariate regression analysis was used to assess the association of several variables with survival while controlling for confounding variables.
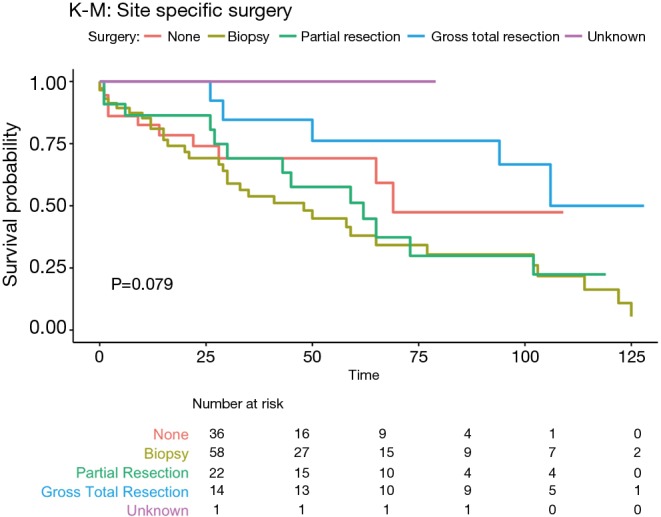
Results: Analysis by multivariate regression of 131 cases showed that increasing age of diagnosis [hazard ratio (HR) 1.52, 95% CI: 1.17-1.99, P=0.001], WHO grade IV classification (HR 8.85, 95% CI: 2.83-27.69, P<0.001), tumor invasiveness (HR 2.94, 95% CI: 1.00-8.64, P=0.047), and sub-total resection (HR 5.80, 95% CI: 1.20-28.03, P=0.029) were associated with statistically significant decreases in survival.
Conclusions: This study suggest that older age, higher WHO grade, tumor invasiveness as well as sub-total resection were all associated with a worse prognosis.
Keywords: Adult; astrocytoma; intradural; intramedullary; oncology; spinal.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Pediatric spinal cord astrocytomas: a retrospective study of 348 patients from the SEER database.J Neurosurg Pediatr. 2017 Jun;19(6):711-719. doi: 10.3171/2017.1.PEDS16528. Epub 2017 Mar 31. J Neurosurg Pediatr. 2017. PMID: 28362182
-
Adult Spinal Ependymomas: An Epidemiologic Study.World Neurosurg. 2018 Mar;111:e53-e61. doi: 10.1016/j.wneu.2017.11.165. Epub 2017 Dec 7. World Neurosurg. 2018. PMID: 29225135
-
Low-grade astrocytomas: the prognostic value of fibrillary, gemistocytic, and protoplasmic tumor histology.J Neurosurg. 2013 Aug;119(2):434-41. doi: 10.3171/2013.4.JNS122329. Epub 2013 May 10. J Neurosurg. 2013. PMID: 23662821
-
Surgical outcomes of pediatric spinal cord astrocytomas: systematic review and meta-analysis.J Neurosurg Pediatr. 2018 Oct;22(4):404-410. doi: 10.3171/2018.4.PEDS17587. Epub 2018 Jul 20. J Neurosurg Pediatr. 2018. PMID: 30028275
-
Primary Spinal Astrocytomas: A Literature Review.Cureus. 2019 Jul 26;11(7):e5247. doi: 10.7759/cureus.5247. Cureus. 2019. PMID: 31565645 Free PMC article. Review.
Cited by
-
Surgical approaches to intramedullary spinal cord astrocytomas in the age of genomics.Front Oncol. 2022 Sep 6;12:982089. doi: 10.3389/fonc.2022.982089. eCollection 2022. Front Oncol. 2022. PMID: 36147920 Free PMC article. Review.
-
Multifocal spinal glioblastoma and leptomeningeal carcinomatosis in an elderly male with hydrocephalus and myelopathy.Surg Neurol Int. 2021 Dec 8;12:595. doi: 10.25259/SNI_985_2021. eCollection 2021. Surg Neurol Int. 2021. PMID: 34992912 Free PMC article.
-
Analyses of DNA Methylation Profiling in the Diagnosis of Intramedullary Astrocytomas.J Neuropathol Exp Neurol. 2021 Aug 11;80(7):663-673. doi: 10.1093/jnen/nlab052. J Neuropathol Exp Neurol. 2021. PMID: 34363673 Free PMC article.
-
Effect of race, sex, and socioeconomic factors on overall survival following the resection of intramedullary spinal cord tumors.J Neurooncol. 2023 Aug;164(1):75-85. doi: 10.1007/s11060-023-04373-9. Epub 2023 Jul 21. J Neurooncol. 2023. PMID: 37479956
-
Impact of Racial Disparities on All-Cause Mortality in Patients With Tumors of the Spinal Cord or Spinal Meninges: A Propensity-Score Analysis.Global Spine J. 2023 Jun;13(5):1365-1373. doi: 10.1177/21925682211033827. Epub 2021 Jul 28. Global Spine J. 2023. PMID: 34318727 Free PMC article.
References
LinkOut - more resources
Full Text Sources