

Acute post-operative airway complications following anterior cervical spine surgery and the role for cricothyrotomy
- PMID: 31032449
- PMCID: PMC6465475
- DOI: 10.21037/jss.2019.03.01
Acute post-operative airway complications following anterior cervical spine surgery and the role for cricothyrotomy
Abstract
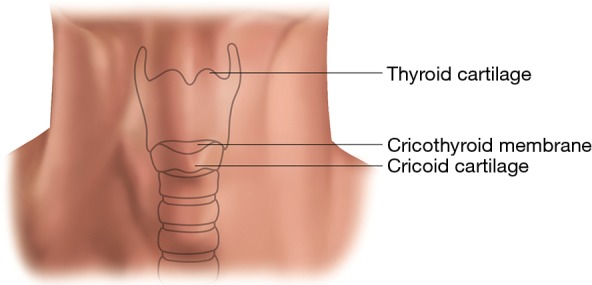
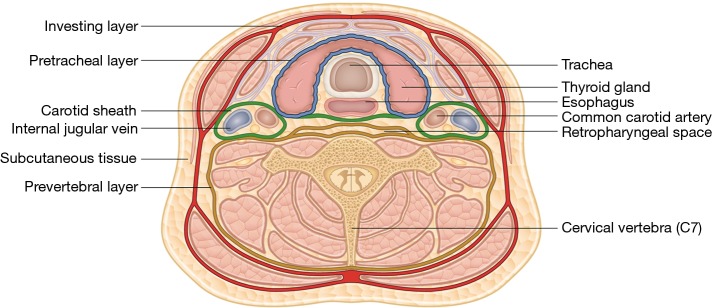
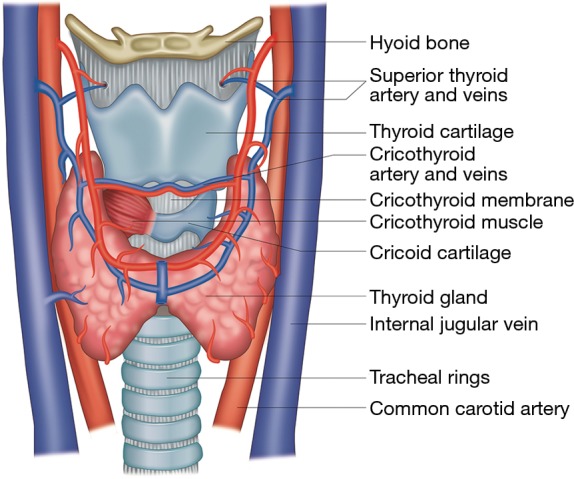
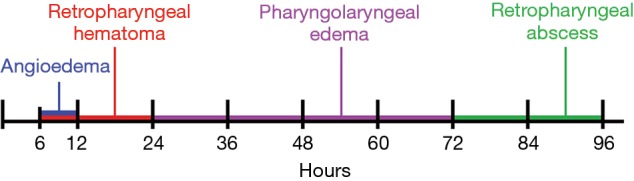
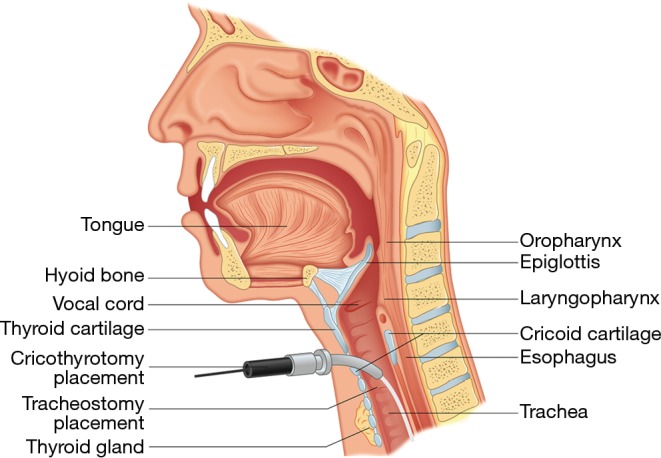
Anterior cervical spine surgery (ACSS) is a common procedure, but not without its own risks and complications. Complications that can cause airway compromise occur infrequently, but can rapidly lead to respiratory arrest, leading to severe morbidity or death. Knowing emergent post-operative airway management including surgical airway placement is critical. We aim to review the different etiologies of post-operative airway compromise following ACSS, the predictable timeline in which they occur, and the most appropriate treatment and management for each. We place special emphasis on the timing and proper surgical technique for an emergent cricothyrotomy. Angioedema is seen the earliest as a cause of post-operative airway compromise, typically within 6-12 hours. Retropharyngeal hematomas can be seen between 6-24 hours, most commonly within 12 hours. Pharyngolaryngeal edema is seen within 24-72 hours. After 72 hours, retropharyngeal abscess is the most likely etiology. Several studies have utilized delayed extubation protocols following ACSS based on patient risk factors and found reduced postoperative airway complications and reintubation rates. The administration of perioperative corticosteroids continues to be controversial with high-level studies recommending both for and against their use. Animal studies showed that after cardiac arrest, the brain can recover if oxygenation is restored within 5 minutes, but this time is likely shorter with asphyxia prior to cardiac arrest. Experience and training are essential to reduce the time for successful cricothyrotomy placement. Physicians must be prepared to diagnose and treat acute postoperative airway complications following ACSS to prevent anoxic brain injury or death. If emergent intubation cannot be accomplished on the first attempt, physicians should not delay placement of a surgical airway such as cricothyrotomy.
Keywords: Anterior cervical spine surgery (ACSS); cricothyrotomy; pharyngolaryngeal edema; post-operative airway compromise; resuscitation; retropharyngeal hematoma.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- Rhee J, Voyadzis JM. Anterior Cervical Diskectomy and Fusion. In: Surgical Anatomy and Techniques to the Spine. 2014:131-8.
-
- Helgeson MD, Albert TJ. Anterior surgical approach to the cervical spine. In: Shen FH, Samartzis D, Fessler RG, editors. Textbook of the Cervical Spine. 1st edition. Philadelphia: Saunders Elsevier; 2014. p. 33-8.
-
- Wilson AS, Samartzis D, Shen FH. Anterior Cervical Diskectomy and Fusion. In: Textbook of the Cervical Spine. 2015:285-93.
Publication types
LinkOut - more resources
Full Text Sources