

Low Body Mass Index Is Associated with Higher Odds of COPD and Lower Lung Function in Low- and Middle-Income Countries
- PMID: 31032662
- PMCID: PMC8579126
- DOI: 10.1080/15412555.2019.1589443
Low Body Mass Index Is Associated with Higher Odds of COPD and Lower Lung Function in Low- and Middle-Income Countries
Abstract
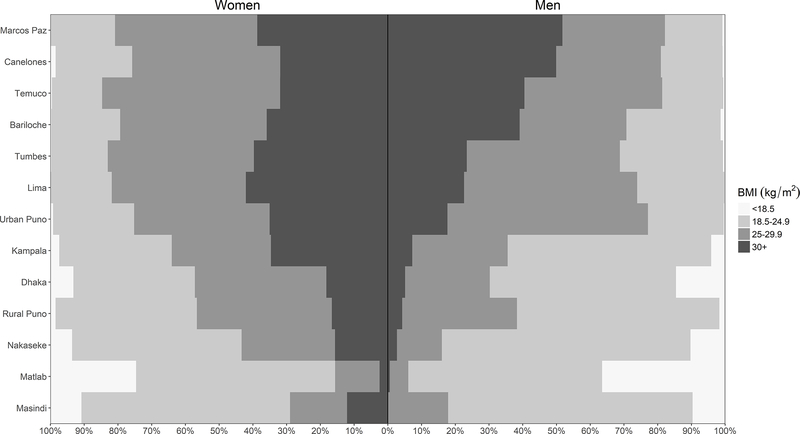
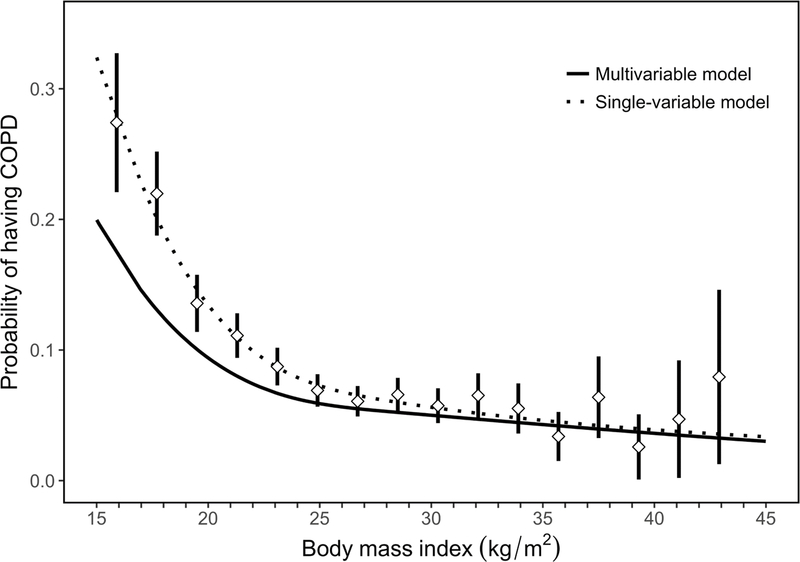
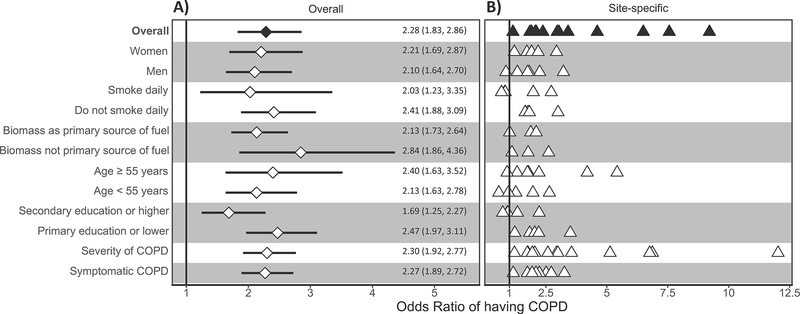
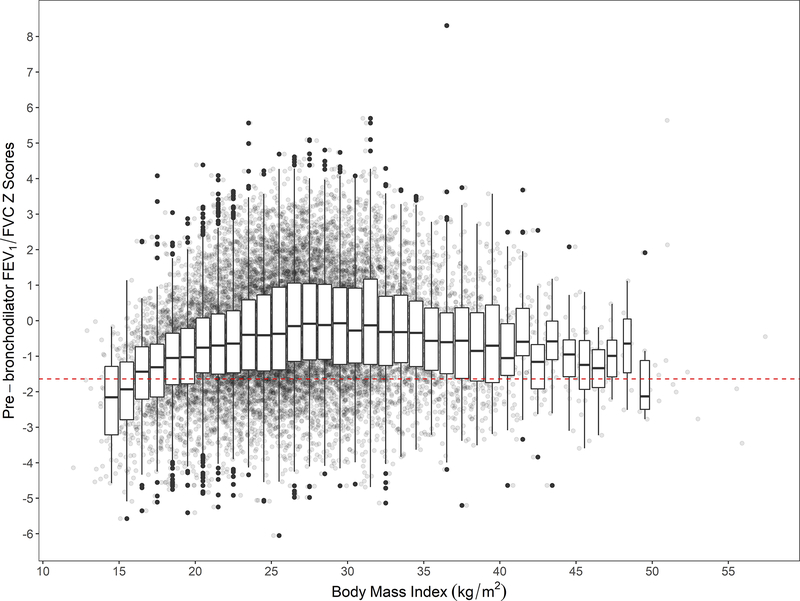
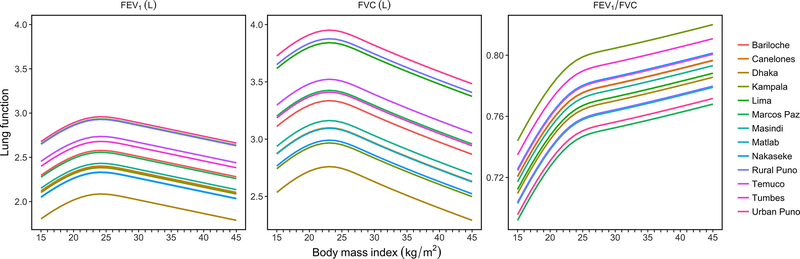
The relationship of body mass index (BMI) with lung function and COPD has been previously described in several high-income settings. However, few studies have examined this relationship in resource-limited settings where being underweight is more common. We evaluated the association between BMI and lung function outcomes across 14 diverse low- and middle-income countries. We included data from 12,396 participants aged 35-95 years and used multivariable regressions to assess the relationship between BMI with either COPD and lung function while adjusting for known risk factors. An inflection point was observed at a BMI of 19.8 kg/m2. Participants with BMI < 19.8 kg/m2 had a 2.28 greater odds (95% CI 1.83-2.86) of having COPD and had a 0.21 (0.13-0.30) lower FEV1 and 0.34 (0.27-0.41) lower FEV1/FVC z-score compared to those with BMI ≥ 19.8 kg/m2. The association with lung function remained even after excluding participants with COPD. Individuals with lower BMI were more likely to have COPD and had lower lung function compared to those in higher BMI. The association with lung function remained positive even after excluding participants with COPD, suggesting that being underweight may also play a role in having worse lung function.
Keywords: COPD; body mass index; low and middle income countries; lung function.
Figures
Similar articles
-
Association between Household Air Pollution Exposure and Chronic Obstructive Pulmonary Disease Outcomes in 13 Low- and Middle-Income Country Settings.Am J Respir Crit Care Med. 2018 Mar 1;197(5):611-620. doi: 10.1164/rccm.201709-1861OC. Am J Respir Crit Care Med. 2018. PMID: 29323928 Free PMC article.
-
Lifetime Body Mass Index Trajectories and Contrasting Lung Function Abnormalities in Mid-Adulthood: Data From the Tasmanian Longitudinal Health Study.Respirology. 2025 Mar;30(3):230-241. doi: 10.1111/resp.14882. Epub 2025 Jan 26. Respirology. 2025. PMID: 39865446 Free PMC article.
-
Gender modifies the effect of body mass index on lung function decline in mild-to-moderate COPD patients: a pooled analysis.Respir Res. 2021 Feb 18;22(1):59. doi: 10.1186/s12931-021-01656-5. Respir Res. 2021. PMID: 33602241 Free PMC article.
-
Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research - a consensus document from six scientific societies.Int J Chron Obstruct Pulmon Dis. 2017 Aug 29;12:2593-2610. doi: 10.2147/COPD.S132236. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28919728 Free PMC article. Review.
-
BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: a meta-analysis of clinical trials.Respir Res. 2019 Oct 29;20(1):236. doi: 10.1186/s12931-019-1209-5. Respir Res. 2019. PMID: 31665000 Free PMC article.
Cited by
-
The Relationship Between BMI and Lung Function in Populations with Different Characteristics: A Cross-Sectional Study Based on the Enjoying Breathing Program in China.Int J Chron Obstruct Pulmon Dis. 2022 Oct 18;17:2677-2692. doi: 10.2147/COPD.S378247. eCollection 2022. Int J Chron Obstruct Pulmon Dis. 2022. PMID: 36281228 Free PMC article.
-
Development and validation of a nomogram for predicting COPD: A nationwide population-based study in South Korea.Medicine (Baltimore). 2024 Sep 27;103(39):e39901. doi: 10.1097/MD.0000000000039901. Medicine (Baltimore). 2024. PMID: 39331887 Free PMC article.
-
Body mass index trajectories in older adulthood and all-cause mortality: a cohort study in China.BMC Public Health. 2025 Apr 7;25(1):1311. doi: 10.1186/s12889-025-22458-0. BMC Public Health. 2025. PMID: 40197247 Free PMC article.
-
Association between appendicular lean mass and chronic obstructive pulmonary disease: epidemiological cross-sectional study and bidirectional Mendelian randomization analysis.Front Nutr. 2023 Jun 29;10:1159949. doi: 10.3389/fnut.2023.1159949. eCollection 2023. Front Nutr. 2023. PMID: 37457977 Free PMC article.
-
Lung function of tuberculosis patients after completion of treatment in Sidama, South Ethiopia.Front Med (Lausanne). 2025 Mar 18;12:1451861. doi: 10.3389/fmed.2025.1451861. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40171505 Free PMC article.
References
-
- Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004; 350:1005–1012. - PubMed
-
- Vestbo J, Hurd SS, Agusti AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 2003; 187:347–365. - PubMed
-
- Burney P, Jarvis D, Perez-Padilla R. The global burden of chronic respiratory disease in adults. Int J Tuberc Lung Dis 2015; 19: 10–20. - PubMed
-
- Garcia-Aymerich J, Gómez FP, Benet M, et al.; PAC-COPD Study Group. Identification and prospective validation of clinically relevant chronic obstructive pulmonary disease (COPD) subtypes. Thorax 2011; 66: 430–437. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical