

Association between Lifelong Physical Activity and Disease Characteristics in HCM
- PMID: 31033902
- PMCID: PMC6798742
- DOI: 10.1249/MSS.0000000000002015
Association between Lifelong Physical Activity and Disease Characteristics in HCM
Abstract
Purpose: Hypertrophic cardiomyopathy (HCM) is characterized by inappropriate left ventricular (LV) wall thickness. Adaptations to exercise can occasionally mimic certain HCM characteristics. However, it is unclear whether physical activity affects HCM genotype expression and disease characteristics. Consequently, we compared lifelong physical activity volumes between HCM gene carriers with and without HCM phenotype, and compared disease characteristics among tertiles of physical activity in phenotypic HCM patients.
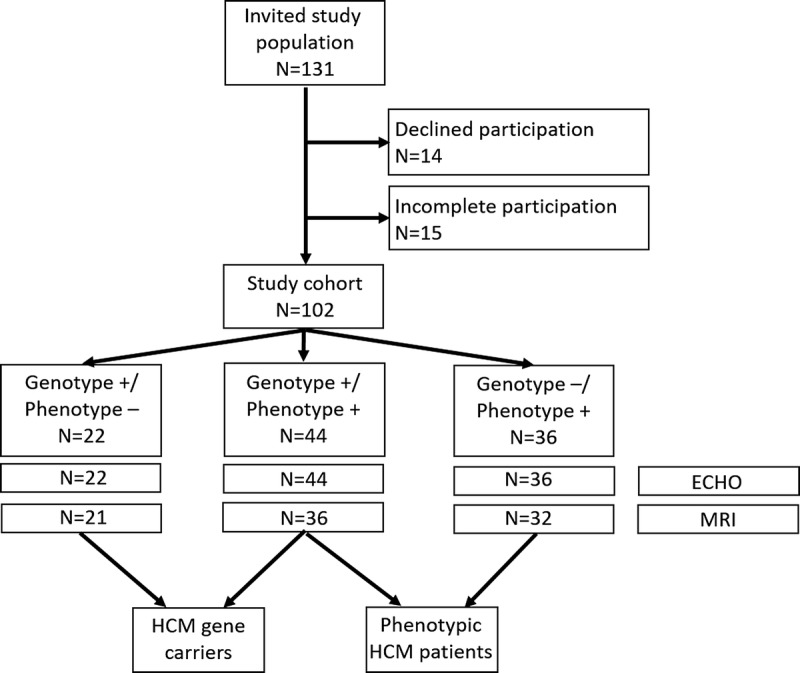
Methods: We enrolled n = 22 genotype positive/phenotype negative (G+/P-) HCM gene carriers, n = 44 genotype positive/phenotype positive (G+/P+) HCM patients, and n = 36 genotype negative/phenotype positive (G-/P+) HCM patients. Lifelong physical activity was recorded using a questionnaire and quantified as metabolic equivalent of task hours per week.
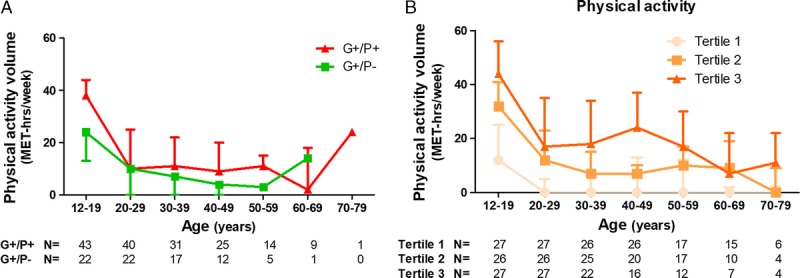
Results: We included 102 participants (51 ± 16 yr, 49% male). Lifelong physical activity volumes were not different between G+/P+ and G+/P- subjects (16 [10-29] vs 14 [6-26] metabolic equivalent of task-hours per week, P = 0.33). Among phenotypic HCM patients, there was no difference in LV wall thickness, mass, and late gadolinium enhancement across physical activity tertiles. Patients with the highest reported physical activity volumes were younger at the time of diagnosis (tertile 1: 52 ± 14 yr, tertile 2: 49 ± 15 yr, tertile 3: 41 ± 18 yr; P = 0.03), and more often had a history of nonsustained ventricular tachycardia (4% vs 30% vs 30%, P = 0.03).
Conclusions: Lifelong physical activity volumes are not associated with genotype-to-phenotype transition in HCM gene carriers. We also found no difference in LV wall thickness across physical activity tertiles. However, the most active HCM patients were younger at the time of diagnosis and had a higher arrhythmic burden. These observations warrant further exploration of the role of exercise in HCM disease development.
Figures
References
-
- Eijsvogels TM, Molossi S, Lee DC, Emery MS, Thompson PD. Exercise at the extremes: the amount of exercise to reduce cardiovascular events. J Am Coll Cardiol. 2016;67(3):316–29. - PubMed
-
- Pluim BM, Zwinderman AH, van der Laarse A, van der Wall EE. The athlete’s heart. A meta-analysis of cardiac structure and function. Circulation. 2000;101(3):336–44. - PubMed
-
- Sharma S, Merghani A, Mont L. Exercise and the heart: the good, the bad, and the ugly. Eur Heart J. 2015;36(23):1445–53. - PubMed
-
- Mazzanti A, Ng K, Faragli A, et al. Arrhythmogenic right ventricular cardiomyopathy: clinical course and predictors of arrhythmic risk. J Am Coll Cardiol. 2016;68(23):2540–50. - PubMed
