

Evaluation of the Diagnostic Stability of the Early Autism Spectrum Disorder Phenotype in the General Population Starting at 12 Months
- PMID: 31034004
- PMCID: PMC6547081
- DOI: 10.1001/jamapediatrics.2019.0624
Evaluation of the Diagnostic Stability of the Early Autism Spectrum Disorder Phenotype in the General Population Starting at 12 Months
Erratum in
-
Typographical Error in the Abstract.JAMA Pediatr. 2019 Aug 1;173(8):801. doi: 10.1001/jamapediatrics.2019.2182. JAMA Pediatr. 2019. PMID: 31233097 Free PMC article. No abstract available.
Abstract
Importance: Universal early screening for autism spectrum disorder (ASD) in primary care is becoming increasingly common and is believed to be a pivotal step toward early treatment. However, the diagnostic stability of ASD in large cohorts from the general population, particularly in those younger than 18 months, is unknown. Changes in the phenotypic expression of ASD across early development compared with toddlers with other delays are also unknown.
Objectives: To examine the diagnostic stability of ASD in a large cohort of toddlers starting at 12 months of age and to compare this stability with that of toddlers with other disorders, such as developmental delay.
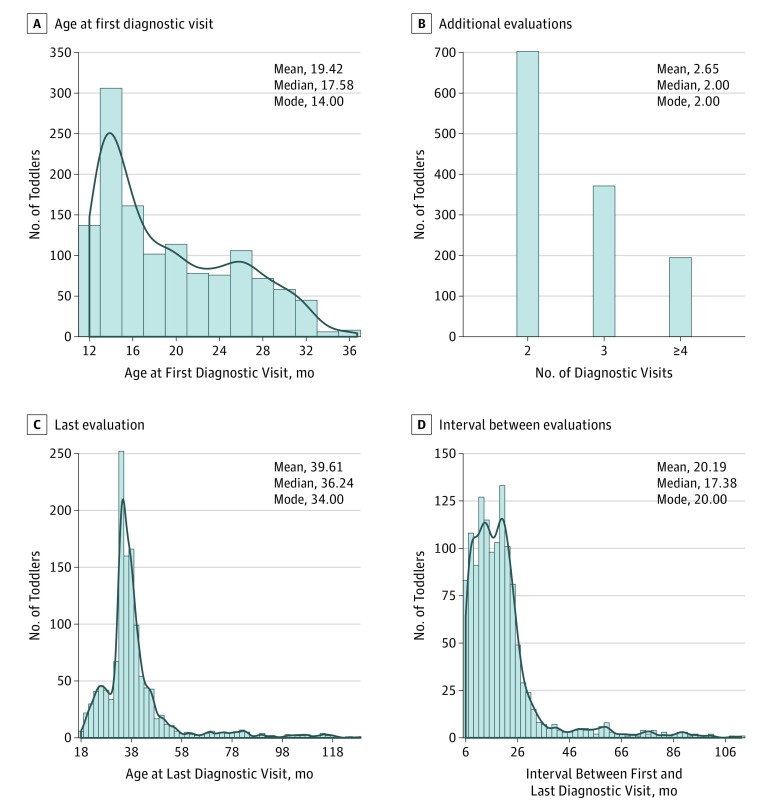
Design, setting, and participants: In this prospective cohort study performed from January 1, 2006, to December 31, 2018, a total of 2241 toddlers were referred from the general population through a universal screening program in primary care or community referral. Eligible toddlers received their first diagnostic evaluation between 12 and 36 months of age and had at least 1 subsequent evaluation.
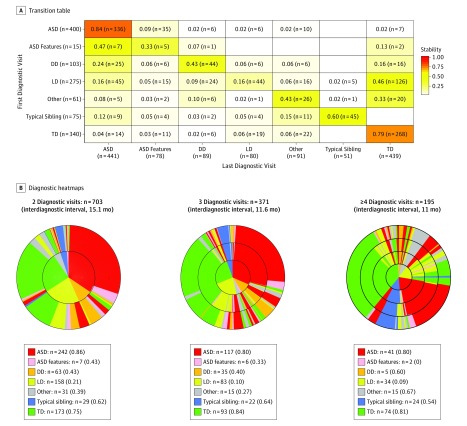
Exposures: Diagnosis was denoted after each evaluation visit as ASD, ASD features, language delay, developmental delay, other developmental issue, typical sibling of an ASD proband, or typical development.
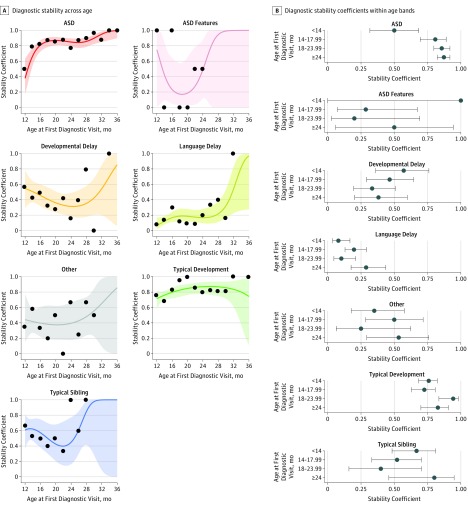
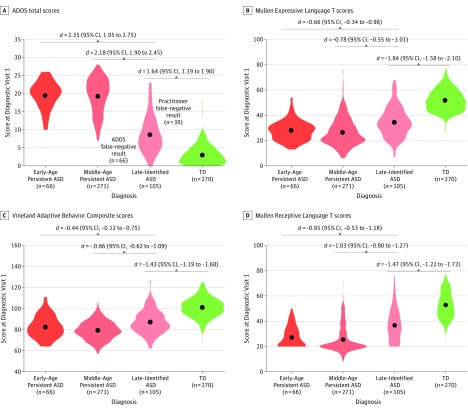
Main outcomes and measures: Diagnostic stability coefficients were calculated within 2-month age bands, and logistic regression models were used to explore the associations of sex, age, diagnosis at first visit, and interval between first and last diagnosis with stability. Toddlers with a non-ASD diagnosis at their first visit diagnosed with ASD at their last were designated as having late-identified ASD.
Results: Among the 1269 toddlers included in the study (918 [72.3%] male; median age at first evaluation, 17.6 months [interquartile range, 14.0-24.4 months]; median age at final evaluation, 36.2 months [interquartile range, 33.4-40.9 months]), the overall diagnostic stability for ASD was 0.84 (95% CI, 0.80-0.87), which was higher than any other diagnostic group. Only 7 toddlers (1.8%) initially considered to have ASD transitioned into a final diagnosis of typical development. Diagnostic stability of ASD within the youngest age band (12-13 months) was lowest at 0.50 (95% CI, 0.32-0.69) but increased to 0.79 by 14 months and 0.83 by 16 months (age bands of 12 vs 14 and 16 months; odds ratio, 4.25; 95% CI, 1.59-11.74). A total of 105 toddlers (23.8%) were not designated as having ASD at their first visit but were identified at a later visit.
Conclusions and relevance: The findings suggest that an ASD diagnosis becomes stable starting at 14 months of age and overall is more stable than other diagnostic categories, including language or developmental delay. After a toddler is identified as having ASD, there may be a low chance that he or she will test within typical levels at 3 years of age. This finding opens the opportunity to test the impact of very early-age treatment of ASD.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
