

Effect of Gastric Residual Evaluation on Enteral Intake in Extremely Preterm Infants: A Randomized Clinical Trial
- PMID: 31034045
- PMCID: PMC6547072
- DOI: 10.1001/jamapediatrics.2019.0800
Effect of Gastric Residual Evaluation on Enteral Intake in Extremely Preterm Infants: A Randomized Clinical Trial
Erratum in
-
Error in Abstract and Results.JAMA Pediatr. 2019 Jun 1;173(6):610. doi: 10.1001/jamapediatrics.2019.1999. JAMA Pediatr. 2019. PMID: 31157871 Free PMC article. No abstract available.
Abstract
Importance: Evaluating prefeed gastric residuals is considered routine care but has little supporting evidence.
Objective: To determine the effect of omitting prefeed gastric residual evaluation on nutritional outcomes in extremely preterm infants.
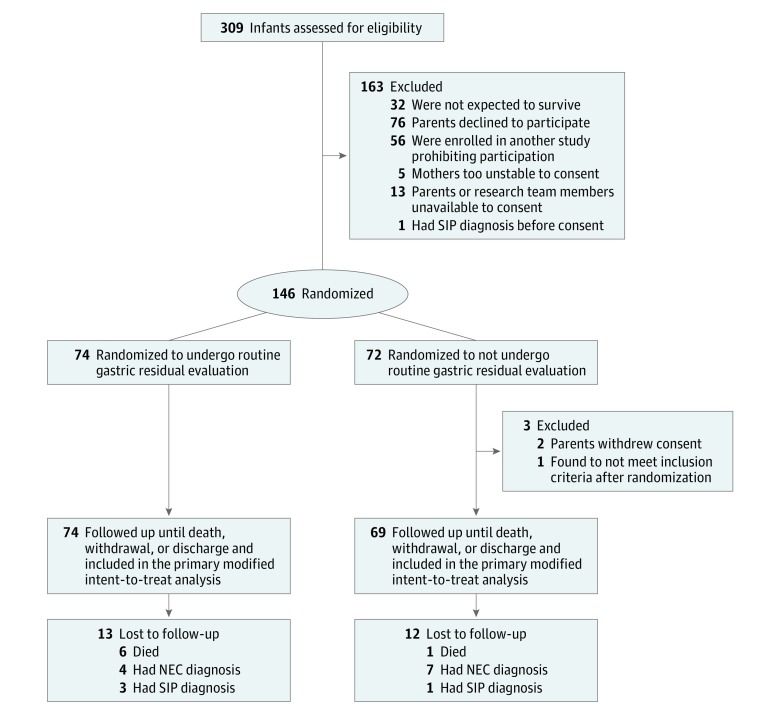
Design, setting, and participants: This single-center randomized clinical trial compared the omission of gastric residual evaluation with prefeed gastric residual evaluation. Infants were recruited from a level 4 neonatal intensive care unit and were enrolled from October 17, 2013, to October 8, 2016, and then followed up for 6 weeks after birth. Eligible participants were infants born at 32 or fewer weeks' gestation with a birth weight of 1250 g or less; they were enrolled within 72 hours after birth and within 24 hours after feeding initiation. All participants (N = 143) were included in the modified intent-to-treat analysis, which was conducted from March to July 2018.
Interventions: The residual group underwent prefeed gastric residual evaluation; the no residual group did not. Feeding decisions were made according to nutritional guidelines, and infants received only human milk.
Main outcomes and measures: The primary outcome was weekly enteral nutrition intake in mL/kg for 6 weeks after birth.
Results: Of 143 infants, 74 (51.7%) were randomized to undergo gastric residual evaluation (residual group) and 69 (48.3%) to omitted gastric residual evaluation (no residual group). The residual group comprised an even number of male and female infants (37 [50.0%]) with a mean (SD) gestational age of 27.1 (2.4) weeks and a mean (SD) birth weight of 888.8 (206.6) grams, whereas the no residual group had more male infants (36 [52.17%]), a mean (SD) gestational age of 27 (1.2) weeks, and a mean (SD) birth weight of 915.2 (180) grams. The no residual group had feedings that advanced more quickly compared with the residual group (mean weekly increase, 20.7 mL/kg/d vs 17.9 mL/kg/d; P = .02) and consumed more feedings at weeks 5 (137.2 [95% CI, 128.6-145.8]; P = .03) and 6 (141.6 [95% CI, 133.2-150.0]; P = .03). Among the secondary outcomes, the no residual group had higher mean estimated log weights (7.01 [95% CI, 6.99-7.02] vs 6.98 [95% CI, 6.97-7.00]; P = .03), had fewer episodes of abdominal distention (0.59 [95% CI, 0.34-1.01] vs 1.79 [95% CI, 1.27-2.53]; P = .001), and were discharged 8 days earlier (4.21 [95% CI, 4.14-4.28] vs 4.28 [95% CI, 4.19-4.36]; P = .01). Odds for necrotizing enterocolitis (0.058 [95% CI, 0.018-0.190] vs 0.026 [95% CI, 0.006-0.109]), death (0.004 [95% CI, 0.0003-0.046] vs 0.012 [95% CI, 0.001-0.131]), late-onset sepsis (0.970 [95% CI, 0.67-1.40] vs 1.38 [95% CI, 0.97-1.94]), and ventilator-associated pneumonia (0.084 [95% CI, 0.033-0.214] vs 0.056 [95% CI, 0.019-0.168]) were similar between groups.
Conclusions and relevance: Among extremely preterm infants, the omission of gastric residual evaluation increased the delivery of enteral nutrition as well as improved weight gain and led to earlier hospital discharge; these results may translate into evidence-based practice.
Trial registration: ClinicalTrials.gov identifier: NCT01863043.
Conflict of interest statement
Figures
Comment in
-
Does prefeed gastric residual evaluation impair enteral nutrition intake in very preterm infants?Acta Paediatr. 2020 Apr;109(4):859-860. doi: 10.1111/apa.15123. Epub 2019 Dec 25. Acta Paediatr. 2020. PMID: 31875649 No abstract available.
-
Is routine evaluation of gastric residuals for premature infants safe or effective?J Perinatol. 2020 Mar;40(3):540-543. doi: 10.1038/s41372-019-0582-8. Epub 2020 Jan 7. J Perinatol. 2020. PMID: 31911644 Free PMC article. No abstract available.
-
Not measuring residual gastric volumes in preterm infants can increase the progression of enteral nutrition with earlier discharge from hospital.Arch Dis Child Educ Pract Ed. 2022 Feb;107(1):77-78. doi: 10.1136/archdischild-2019-318671. Epub 2020 May 27. Arch Dis Child Educ Pract Ed. 2022. PMID: 32461252 No abstract available.
References
-
- McClave SA, Taylor BE, Martindale RG, et al. ; Society of Critical Care Medicine; American Society for Parenteral and Enteral Nutrition . Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. 2016;40(2):159-211. doi:10.1177/0148607115621863 - DOI - PubMed
-
- Mehta NM, Skillman HE, Irving SY, et al. . Guidelines for the provision and assessment of nutrition support therapy in the pediatric critically ill patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. JPEN J Parenter Enteral Nutr. 2017;41(5):706-742. doi:10.1177/0148607117711387 - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
