

Longitudinal Relationship Between Frailty and Cognition in Patients 50 Years and Older with Breast Cancer
- PMID: 31034595
- PMCID: PMC6490967
- DOI: 10.1111/jgs.15934
Longitudinal Relationship Between Frailty and Cognition in Patients 50 Years and Older with Breast Cancer
Abstract
Objectives: To evaluate relationships between frailty and cognition longitudinally in adults 50 years and older with breast cancer receiving chemotherapy.
Design: Secondary analysis of a prospective longitudinal observational study.
Setting: University of Rochester NCI Community Oncology Research Program community oncology clinics.
Participants: Patients with breast cancer age 50 and older receiving adjuvant/neoadjuvant chemotherapy (n = 376) and age-matched controls without cancer (n = 234).
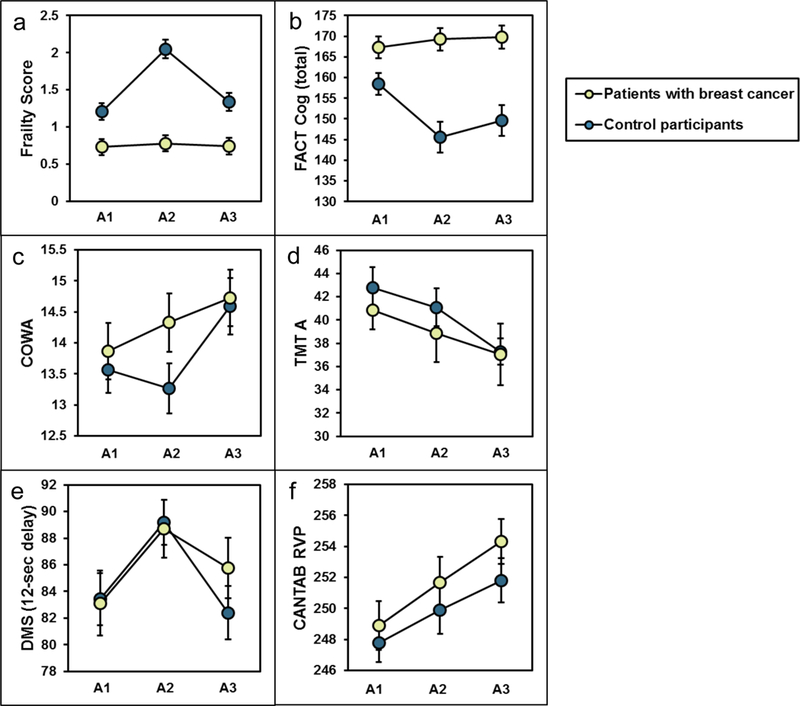
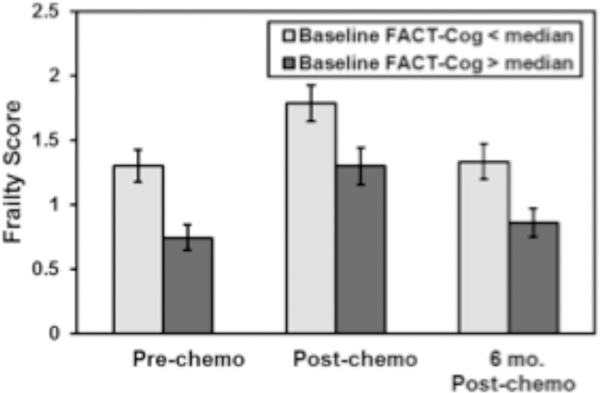
Measurements: Frailty was assessed using a modified frailty score from self-reported assessments (weakness, exhaustion, physical activity, and gait speed). Cognition was assessed by patient report (Functional Assessment of Cancer Therapy-Cognition [FACT-Cog]) and objective measures. Frailty and cognition were measured at three time points (prechemotherapy [A1], postchemotherapy [A2], and 6 months postchemotherapy [A3]; similar time interval for controls). Linear regression models evaluated associations between frailty and cognition adjusting for covariates.
Results: The average age was 59 years (standard deviation = 6.4 y). At baseline, patients with cancer had a higher mean frailty score (1.21 vs .73; P < .001) and lower mean FACT-Cog score (158.4 vs 167.3; P < .001) compared with controls. Objective cognitive measures were not statistically different. Longitudinal decline in FACT-Cog between A1 and A2 (P < .05) and between A1 and A3 (P < .01) was associated with increased frailty score in patients compared with controls. Longitudinal worsening in Controlled Oral Word Association (P < .05) and Trail-Making Test (P < .01) were associated with an increase in frailty between A1 and A2 in patients compared with controls; longitudinal decline in the Delayed Match to Sample test was associated with an increase in frailty between A1 and A3 (P < .05) in patients compared with controls. This finding remained significant for a subset analysis of those aged 65 and older.
Conclusion: In patients with breast cancer aged 50 and older, longitudinal decline in FACT-Cog and objective measures of attention and memory were associated with increased frailty during treatment and up to 6 months posttreatment. Overall, our study suggests cognition and frailty are both important factors to assess in breast cancer patients. J Am Geriatr Soc 67:928-936, 2019.
Trial registration: ClinicalTrials.gov NCT00024102.
Keywords: breast cancer; chemotherapy; cognition; cognitive impairment; frailty.
© 2019 The American Geriatrics Society.
Conflict of interest statement
Conflict of interest
Figures
Similar articles
-
Cognitive Complaints in Survivors of Breast Cancer After Chemotherapy Compared With Age-Matched Controls: An Analysis From a Nationwide, Multicenter, Prospective Longitudinal Study.J Clin Oncol. 2017 Feb 10;35(5):506-514. doi: 10.1200/JCO.2016.68.5826. Epub 2016 Dec 28. J Clin Oncol. 2017. PMID: 28029304 Free PMC article.
-
Physical Frailty Is Associated with Longitudinal Decline in Global Cognitive Function in Non-Demented Older Adults: A Prospective Study.J Nutr Health Aging. 2018;22(1):82-88. doi: 10.1007/s12603-017-0924-1. J Nutr Health Aging. 2018. PMID: 29300426
-
Longitudinal Changes in Cognitive Function in a Nationwide Cohort Study of Patients With Lymphoma Treated With Chemotherapy.J Natl Cancer Inst. 2022 Jan 11;114(1):47-59. doi: 10.1093/jnci/djab133. J Natl Cancer Inst. 2022. PMID: 34255086 Free PMC article.
-
Cognitive effects of cancer and its treatments at the intersection of aging: what do we know; what do we need to know?Semin Oncol. 2013 Dec;40(6):709-25. doi: 10.1053/j.seminoncol.2013.09.006. Semin Oncol. 2013. PMID: 24331192 Free PMC article. Review.
-
Assessing the Current State of Cognitive Frailty: Measurement Properties.J Nutr Health Aging. 2017;21(2):152-160. doi: 10.1007/s12603-016-0735-9. J Nutr Health Aging. 2017. PMID: 28112769 Review.
Cited by
-
Longitudinal Analysis of Patient-Reported Cognitive Function in Multiple Myeloma.Clin Lymphoma Myeloma Leuk. 2022 Dec;22(12):920-927. doi: 10.1016/j.clml.2022.08.002. Epub 2022 Aug 15. Clin Lymphoma Myeloma Leuk. 2022. PMID: 36085276 Free PMC article.
-
Cognitive impairments associated with chemotherapy in women with breast cancer: a meta-analysis and meta-regression.Braz J Med Biol Res. 2023 Oct 13;56:e12947. doi: 10.1590/1414-431X2023e12947. eCollection 2023. Braz J Med Biol Res. 2023. PMID: 37851791 Free PMC article.
-
Physiologic Frailty and Neurocognitive Decline Among Young-Adult Childhood Cancer Survivors: A Prospective Study From the St Jude Lifetime Cohort.J Clin Oncol. 2021 Nov 1;39(31):3485-3495. doi: 10.1200/JCO.21.00194. Epub 2021 Jul 20. J Clin Oncol. 2021. PMID: 34283634 Free PMC article.
-
Longitudinal trajectories of a claims-based frailty measure during adjuvant chemotherapy in women with stage I-III breast cancer.Oncologist. 2024 Oct 3;29(10):e1291-e1301. doi: 10.1093/oncolo/oyae092. Oncologist. 2024. PMID: 38716777 Free PMC article.
-
Associations of frailty with symptoms, and HRQOL in older cancer survivors after cancer treatments: a systematic review and meta-analyses.Qual Life Res. 2024 Mar;33(3):583-598. doi: 10.1007/s11136-023-03537-4. Epub 2023 Oct 28. Qual Life Res. 2024. PMID: 37897643
References
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–156. - PubMed
-
- Rockwood K, Mitnitski A, Song X, Steen B, Skoog I. Long-term risks of death and institutionalization of elderly people in relation to deficit accumulation at age 70. J Am Geriatr Soc. 2006;54(6):975–979. - PubMed
-
- Guerard EJ, Deal AM, Chang Y, et al. Frailty Index Developed From a Cancer-Specific Geriatric Assessment and the Association With Mortality Among Older Adults With Cancer. J Natl Compr Canc Netw. 2017;15(7):894–902. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- U10CA037420/CA/NCI NIH HHS/United States
- DP2 CA195765/CA/NCI NIH HHS/United States
- R21/R33AG059206/CA/NCI NIH HHS/United States
- K07 CA168886/CA/NCI NIH HHS/United States
- UG1CA189961/CA/NCI NIH HHS/United States
- R25CA102618/CA/NCI NIH HHS/United States
- DP2CA195765/CA/NCI NIH HHS/United States
- K24 AG055693/AG/NIA NIH HHS/United States
- UG1 CA189961/CA/NCI NIH HHS/United States
- R33 AG059206/AG/NIA NIH HHS/United States
- U10 CA037420/CA/NCI NIH HHS/United States
- R21 AG059206/AG/NIA NIH HHS/United States
- K07CA168886/CA/NCI NIH HHS/United States
- K24 AG056589/AG/NIA NIH HHS/United States
- R25 CA102618/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
