

Adaptive Changes of Glioblastoma Cells Following Exposure to Hypoxic (1% Oxygen) Tumour Microenvironment
- PMID: 31035344
- PMCID: PMC6539006
- DOI: 10.3390/ijms20092091
Adaptive Changes of Glioblastoma Cells Following Exposure to Hypoxic (1% Oxygen) Tumour Microenvironment
Abstract
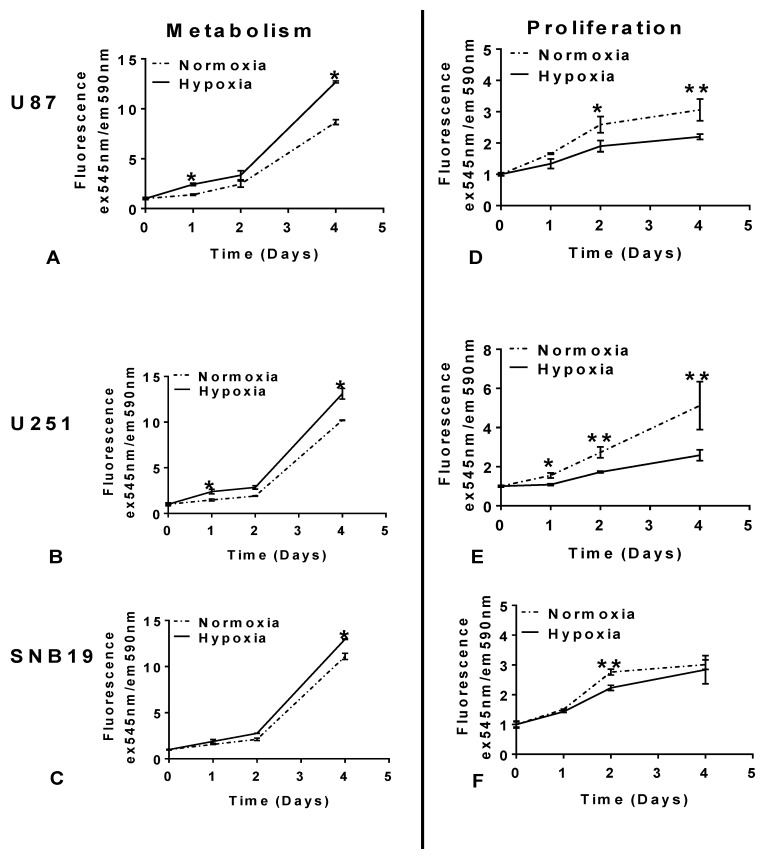
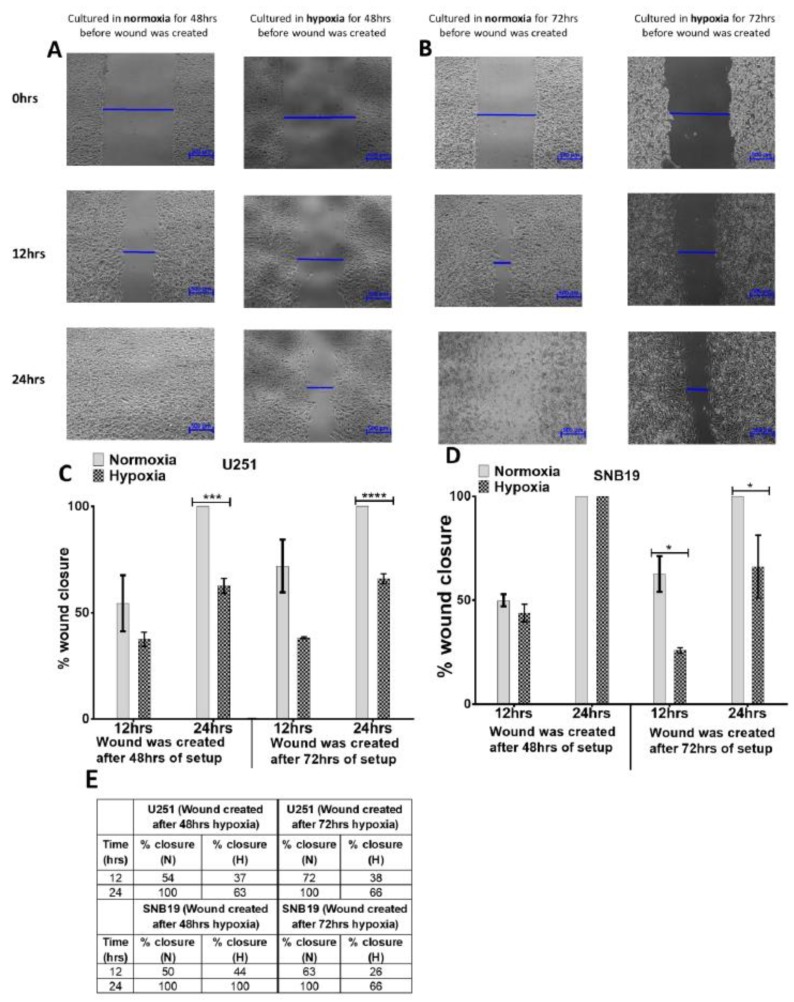
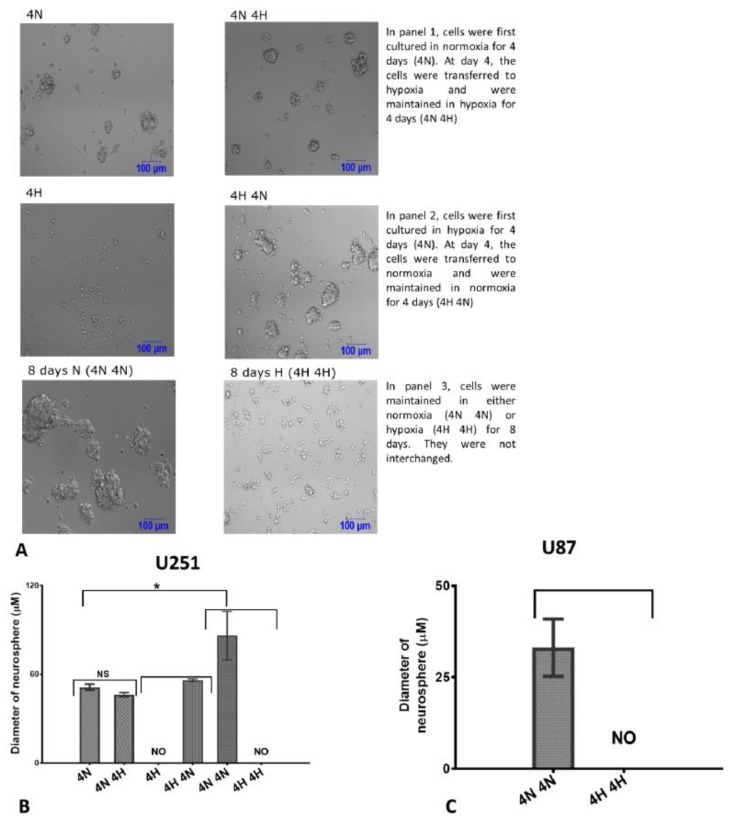
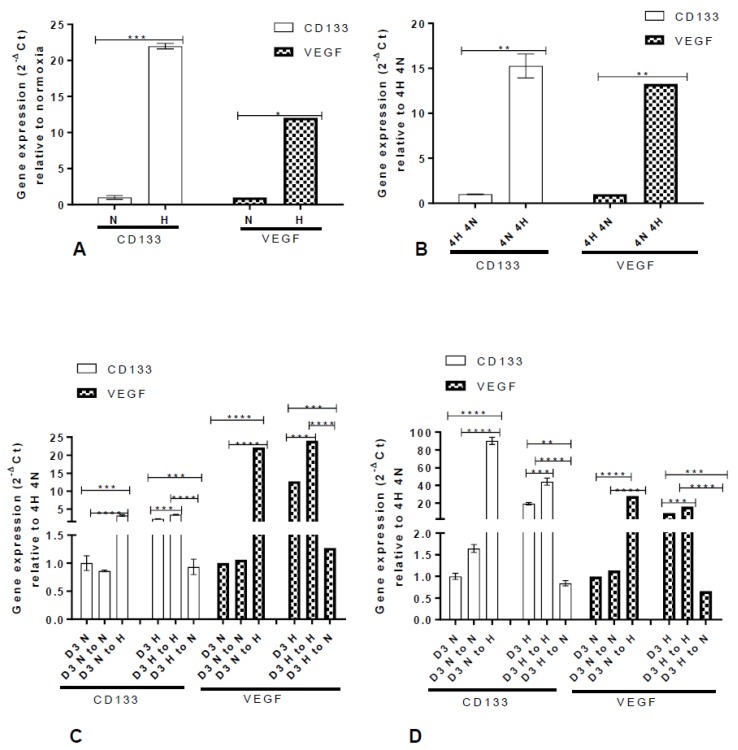
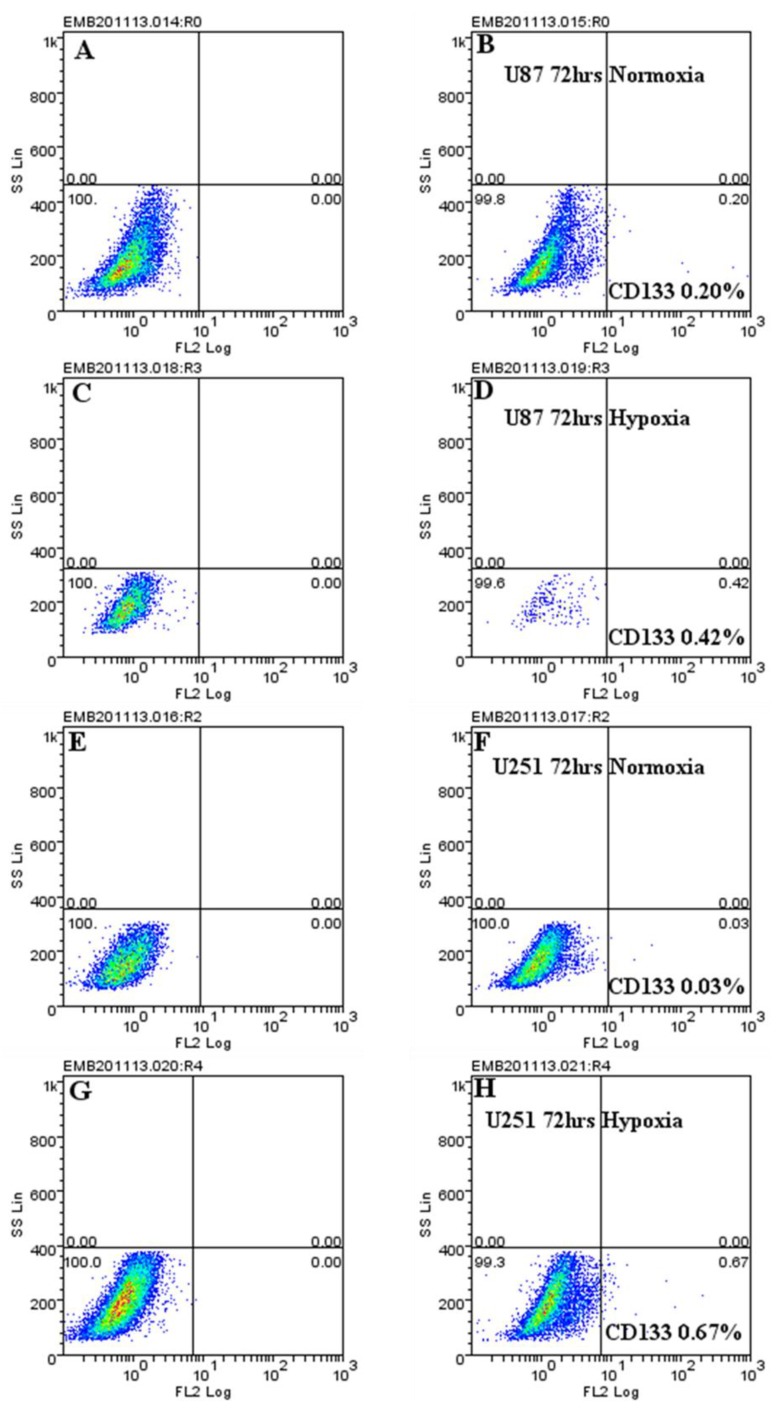
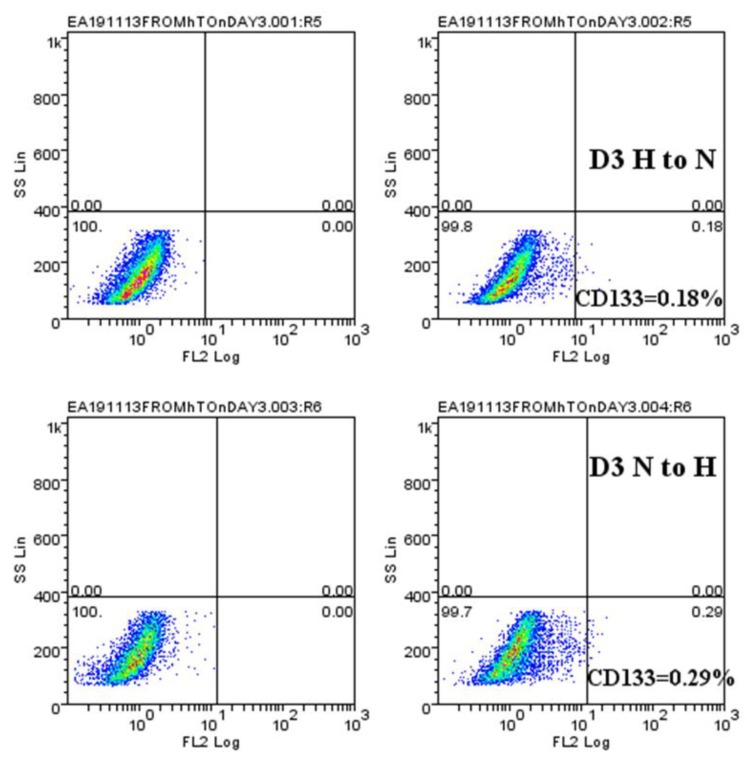
Glioblastoma multiforme is the most aggressive and malignant primary brain tumour, with a median survival rate of between 15 to 17 months. Heterogeneous regions occur in glioblastoma as a result of oxygen gradients which ranges from 0.1% to 10% in vivo. Emerging evidence suggests that tumour hypoxia leads to increased aggressiveness and chemo/radio resistance. Yet, few in vitro studies have been performed in hypoxia. Using three glioblastoma cell-lines (U87, U251, and SNB19), the adaptation of glioblastoma cells in a 1% (hypoxia) and 20% (normoxia) oxygen microenvironment on proliferation, metabolism, migration, neurosphere formation, CD133 and VEGF expression was investigated. Compared to cells maintained in normoxia (20% oxygen), glioblastoma cells adapted to 1% oxygen tension by reducing proliferation and enhancing metabolism. Both migratory tendency and neurosphere formation ability were greatly limited. In addition, hypoxic-mediated gene upregulation (CD133 and VEGF) was reversed when cells were removed from the hypoxic environment. Collectively, our results reveal that hypoxia plays a pivotal role in changing the behaviour of glioblastoma cells. We have also shown that genetic modulation can be reversed, supporting the concept of reversibility. Thus, understanding the degree of oxygen gradient in glioblastoma will be crucial in personalising treatment for glioblastoma patients.
Keywords: CD133; glioblastoma; hypoxia; personalised treatment; tumour microenvironment.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gilbert M.R., Wang M., Aldape K.D., Stupp R., Hegi M.E., Jaeckle K.A., Armstrong T.S., Wefel J.S., Won M., Blumenthal D.T. Dose-dense temozolomide for newly diagnosed glioblastoma: A randomized phase III clinical trial. J. Clin. Oncol. 2013;31:4085. doi: 10.1200/JCO.2013.49.6968. - DOI - PMC - PubMed
-
- Stupp R., Hegi M.E., Mason W.P., van den Bent M.J., Taphoorn M.J., Janzer R.C., Ludwin S.K., Allgeier A., Fisher B., Belanger K. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. doi: 10.1016/S1470-2045(09)70025-7. - DOI - PubMed
-
- Balkwill F.R., Capasso M., Hagemann T. The Tumor Microenvironment at a Glance. The Company of Biologists Ltd.; Cambridge, UK: 2012. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
