

The presence of bacteria varies between colorectal adenocarcinomas, precursor lesions and non-malignant tissue
- PMID: 31035942
- PMCID: PMC6489238
- DOI: 10.1186/s12885-019-5571-y
The presence of bacteria varies between colorectal adenocarcinomas, precursor lesions and non-malignant tissue
Abstract
Background: A causal association has been suggested between certain bacteria and colorectal cancer (CRC). Only a few studies have, however, investigated the presence of these bacteria directly in colon tissue with conflicting results. It is thus uncertain which role they may have in prognosis and carcinogenesis of CRC.
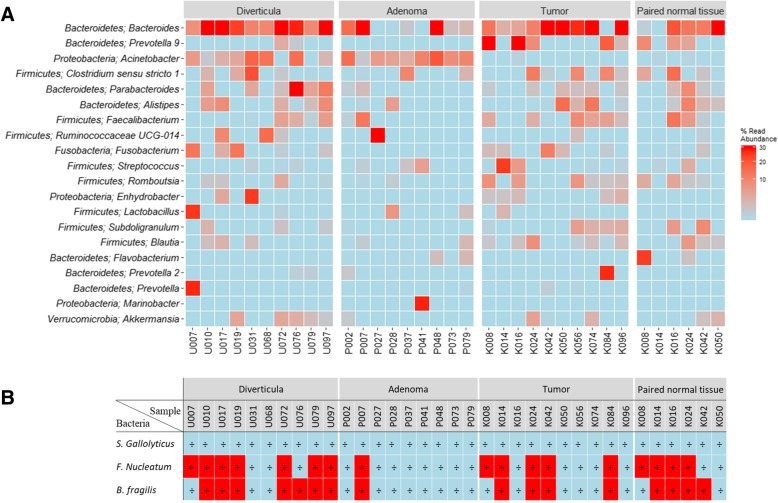
Methods: Formalin-fixed and paraffin-embedded (FFPE) colorectal tissue samples from patients diagnosed with colorectal cancer (CRC)(tumor and paired normal tissue, n = 99), adenomas (n = 96), or diverticular disease (n = 104) were tested for the presence and bacterial load of Streptococcus gallolyticus (S. gallolyticus), Fusobacterium nucleatum (F. nucleatum), and Bacteroides fragilis (B. fragilis) using quantitative PCR. A subsequent broader search was conducted on a subset of samples using 16S ribosomal RNA gene sequencing. Finally, to evaluate the prognostic value, the bacterial status was compared to patient outcome.
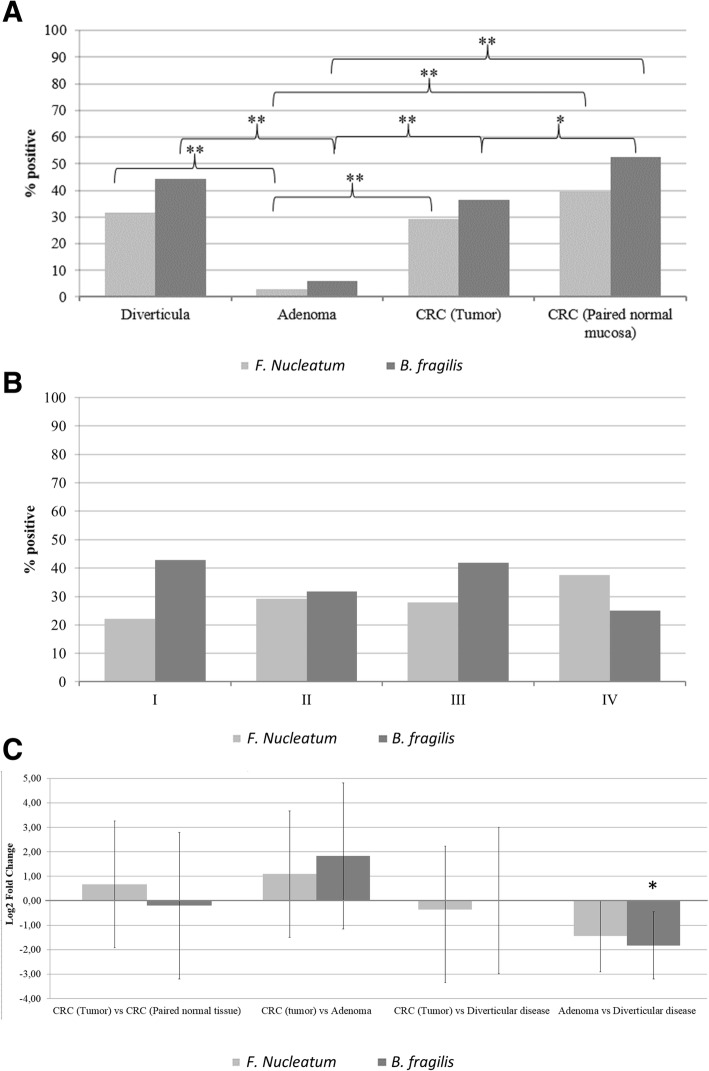
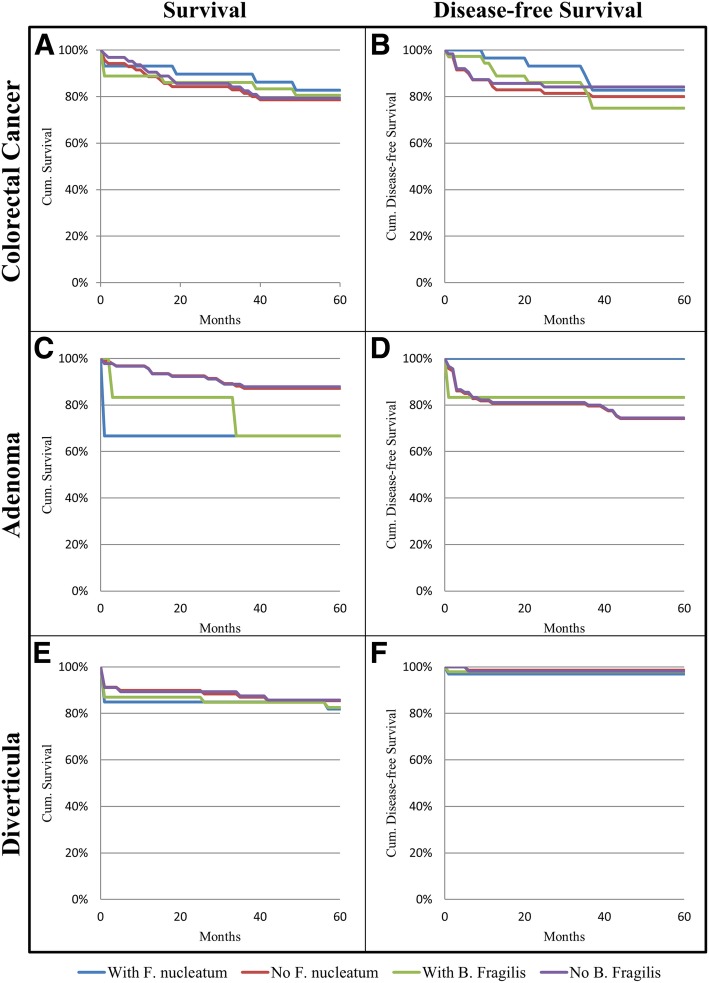
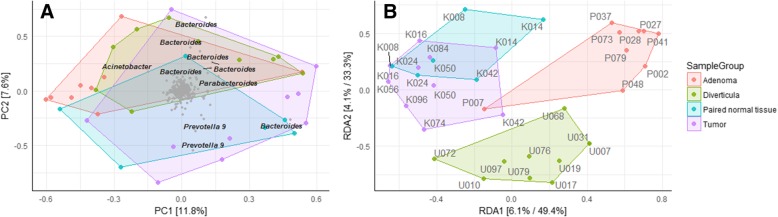
Results: S. gallolyticus was not detected by qPCR in any of the investigated tissue samples and F. nucleatum and B. fragilis were found to be equally distributed in tumors, paired normal tissue, and diverticula, but significantly less present in adenomas compared to both tumors and diverticula. Neither, F. nucleatum nor B. fragilis status affected the five-year prognosis of the patients. The 16S rRNA gene sequencing data revealed that tumors were associated with the Prevotella genus while conversely adenomas and diverticula were associated with Acinetobacter genus.
Conclusion: These findings do not support a role of F. nucleatum or B. fragilis during colorectal beginning, while S. gallolyticus was not implicated in the colorectal tissue of a Danish population. A potential role of the bacterial genera Prevotella and Acinetobacter was indicated, and requires further investigations.
Keywords: Acinetobacter; Bacteroides; Cancer microbiota; Colorectal adenomas; Colorectal cancer; Fusobacterium; Prevotella; Streptococcus.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethical committee of the North Denmark Region (N-20150059) and reported for the Data Protection Agency. All samples were non-traceable, anonymized samples for which the Regional Ethical Committee waived the requirement for informed consent. The investigation has been conducted according to principles expressed in the Declaration of Helsinki.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- L a T, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;00:1–22. - PubMed
-
- Hadac J. N., Leystra A. A., Paul Olson T. J., Maher M. E., Payne S. N., Yueh A. E., Schwartz A. R., Albrecht D. M., Clipson L., Pasch C. A., Matkowskyj K. A., Halberg R. B., Deming D. A. Colon Tumors with the Simultaneous Induction of Driver Mutations in APC, KRAS, and PIK3CA Still Progress through the Adenoma-to-carcinoma Sequence. Cancer Prevention Research. 2015;8(10):952–961. doi: 10.1158/1940-6207.CAPR-15-0003. - DOI - PMC - PubMed
-
- S a B, Day NE, Luben R, Ferrari P, Slimani N, Norat T, et al. Dietary fibre in food and protection against colorectal cancer in the European prospective investigation into Cancer and nutrition (EPIC): an observational study. Lancet. 2003;361:1496–1501. doi: 10.1016/S0140-6736(03)13174-1. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
