

Impact of time to initiation of radiotherapy on survival after resection of newly diagnosed glioblastoma
- PMID: 31036031
- PMCID: PMC6489245
- DOI: 10.1186/s13014-019-1272-6
Impact of time to initiation of radiotherapy on survival after resection of newly diagnosed glioblastoma
Abstract
Background and purpose: To evaluate the effect of timing of radiotherapy (RT) on survival in patients with newly diagnosed primary glioblastoma (GBM) treated with the same therapeutical protocol.
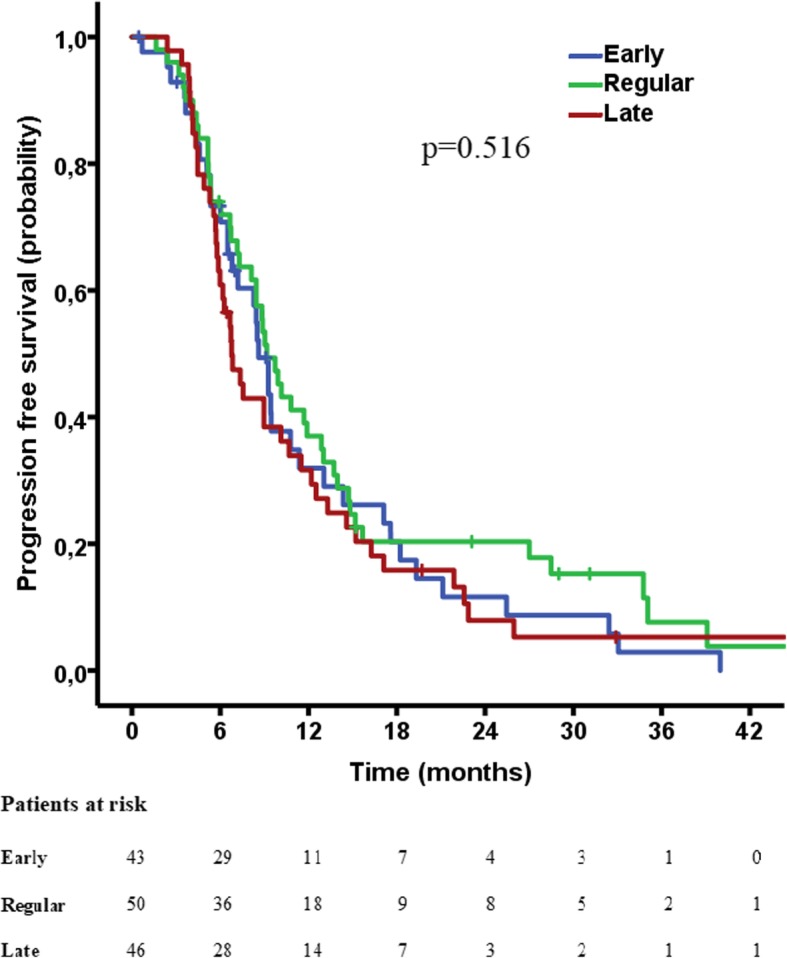
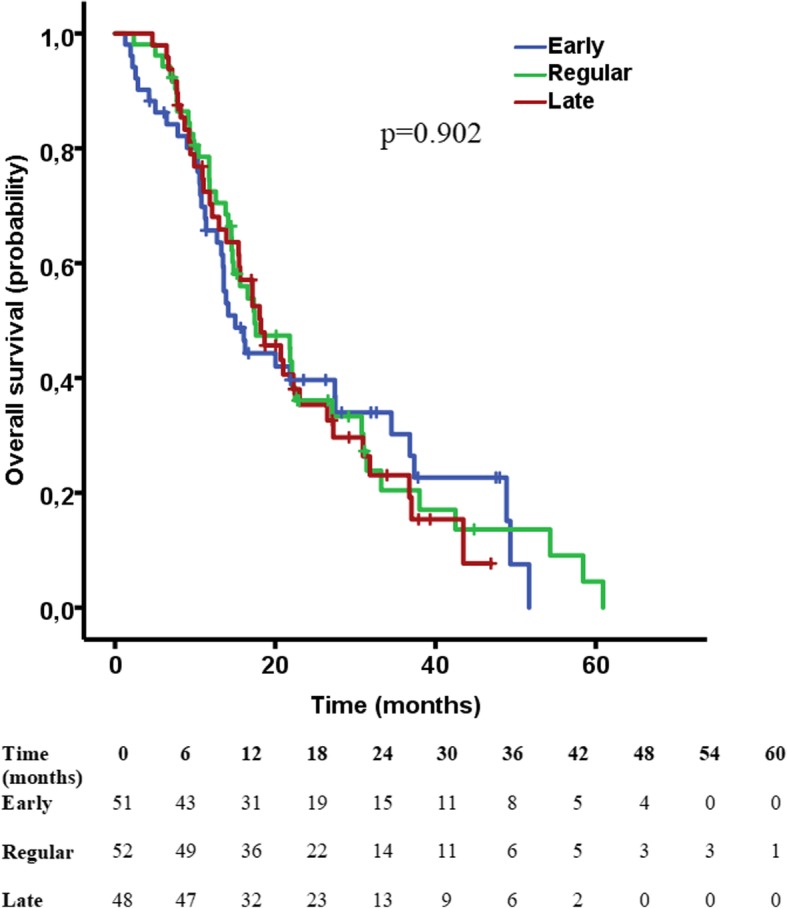
Materials and methods: Patients with newly diagnosed primary GBM treated with the same therapeutical scheme between 2010 and 2015 in our institution were retrospectively reviewed. The population was trichotomized based on the time interval from surgery till initiation of RT (< 28 days, 28-33 days, > 33 days). Kaplan-Meier and Cox regression analyses were used to compare progression free survival (PFS) and overall survival (OS) between the groups. The influence of various extensively studied prognostic factors on survival was assessed by multivariate analysis.
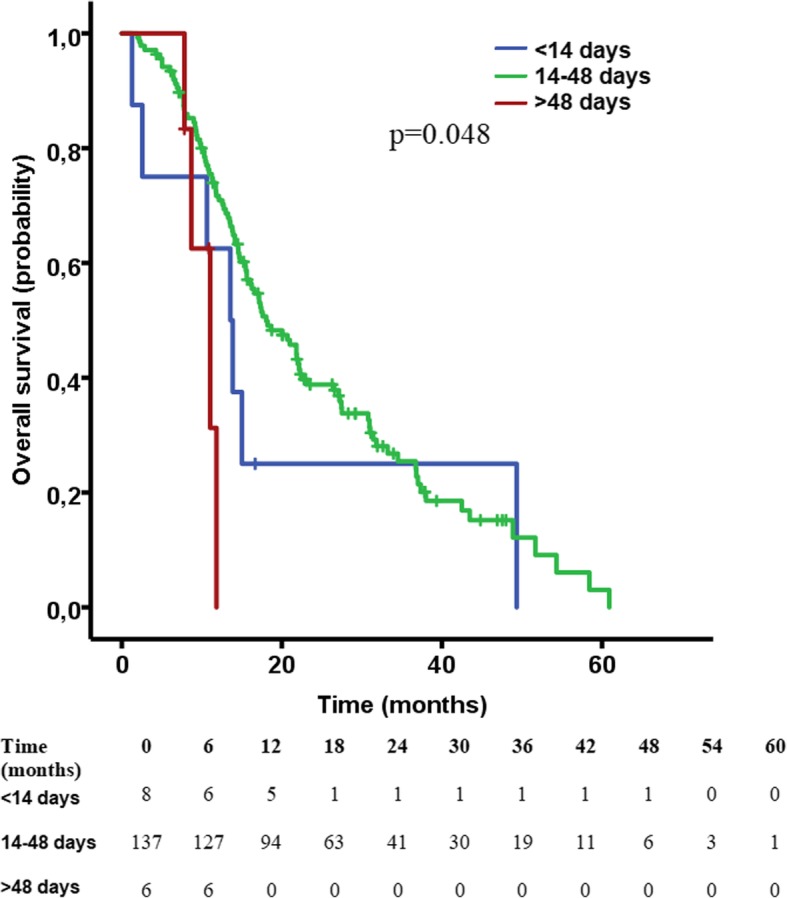
Results: One-hundred-fifty-one patients met the inclusion criteria. Between the three groups no significant difference in PFS (p = 0.516) or OS (p = 0.902) could be demonstrated. Residual tumor volume (RTV) and midline structures involvement were identified as independent prognostic factors of PFS while age, O-6-Methylguanine Methyltransferase (MGMT) status, Ki67 index, RTV and midline structures involvement represented independent predictors of OS. Patients starting RT after a prolonged delay (> 48 days) exhibited a significantly shorter OS (p = 0.034).
Conclusion: Initiation of RT within a timeframe of 48 days is not associated with worsened survival. A prolonged delay (> 48 days) may be associated with worse OS. RT should neither be delayed, nor forced, but should rather start timely, as soon as the patient has recovered from surgery.
Keywords: Glioblastoma; Prognostic factors; Progression free survival; Survival; Timing of radiotherapy.
Conflict of interest statement
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- WHO. World Cancer Report 2014: WHO; 2015. http://publications.iarc.fr/Non-Series-Publications/World-Cancer-Reports....
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
