

Idiopathic and isolated adrenocorticotropic hormone deficiency presenting as continuous epigastric discomfort without symptoms of hypoglycemia: a case report
- PMID: 31036085
- PMCID: PMC6489309
- DOI: 10.1186/s13256-019-2050-7
Idiopathic and isolated adrenocorticotropic hormone deficiency presenting as continuous epigastric discomfort without symptoms of hypoglycemia: a case report
Abstract
Background: Isolated adrenocorticotropic hormone deficiency is one kind of hypopituitarism and is triggered by various diseases including autoimmune disorder and/or autoimmune hypophysitis. Adrenocorticotropic hormone deficiency brings out various serious symptoms such as severe hypoglycemia, hypotensive shock, and disturbance of consciousness.
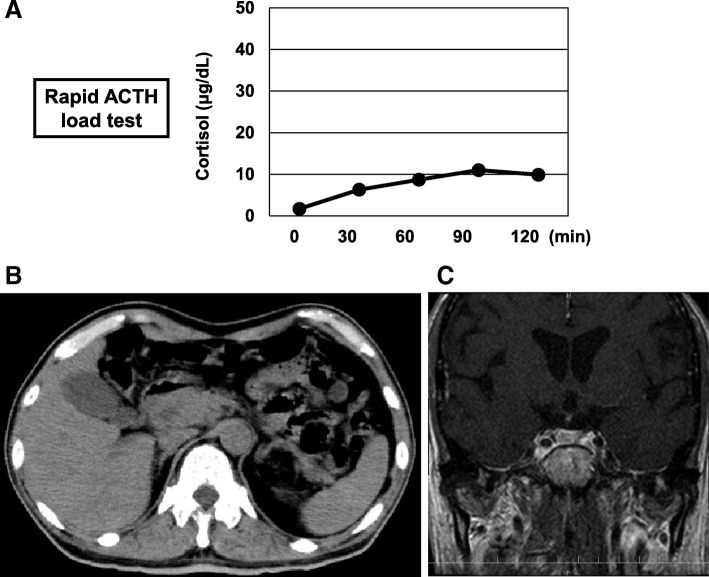
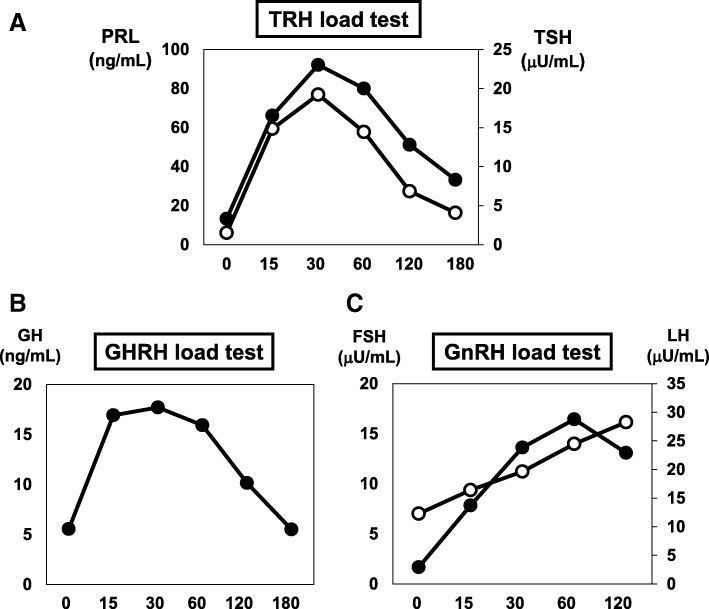
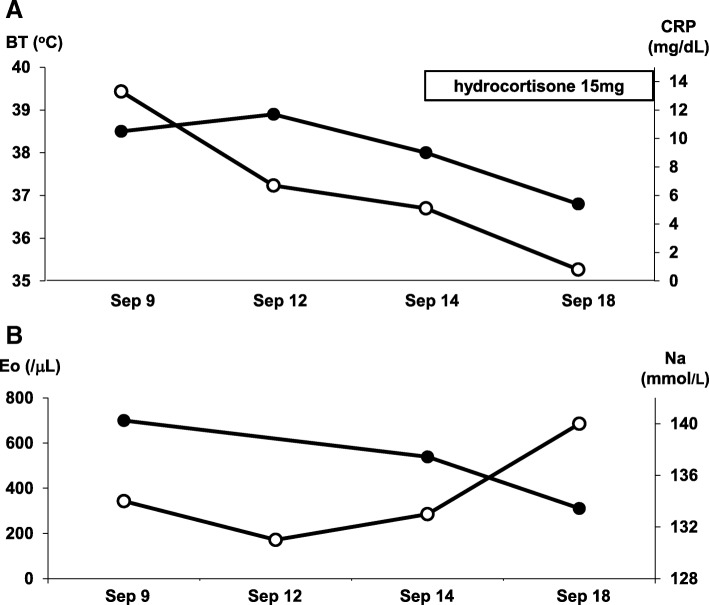
Case presentation: Here we report a case of 65-year-old Japanese man who developed idiopathic and isolated adrenocorticotropic hormone deficiency. He had continued epigastric comfort without any symptom of hypoglycemia or any autoimmune abnormality. Since he continued to complain of mild epigastric discomfort and general malaise, he was misdiagnosed as having functional dyspepsia and a depression state and took medicine for them for several months. Infection markers and several antibodies which we examined were all negative. An abdominal computed tomography scan showed no mass in adrenal tissue; contrast magnetic resonance imaging of his brain showed that pituitary size was within normal range, and pituitary gland deep dyeing delay and/or deeply stained deficit were not observed. However, in a corticotropin-releasing hormone load test, response of adrenocorticotropic hormone and cortisol was poor after corticotropin-releasing hormone loading, and in growth hormone-releasing peptide 2 load test, adrenocorticotropic hormone response was poor, suggesting the presence of adrenocorticotropic hormone deficiency. Therefore, we started treatment with hydrocortisone, and his various symptoms were soon mitigated.
Conclusions: We should bear in mind the possibility of adrenocorticotropic hormone deficiency even when patients complain of epigastric discomfort or general malaise alone.
Keywords: ACTH deficiency; Case report; Epigastric discomfort; General malaise; Hypoglycemia.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Treatable Bedridden Elderly -Recovery from Flexion Contracture after Cortisol Replacement in a Patient with Isolated Adrenocorticotropic Hormone Deficiency.Intern Med. 2016;55(20):2975-2978. doi: 10.2169/internalmedicine.55.6932. Epub 2016 Oct 15. Intern Med. 2016. PMID: 27746435 Free PMC article.
-
Somatic delusions, unusual presenting symptoms of isolated adrenocorticotropin deficiency.Gen Hosp Psychiatry. 2015 Jan-Feb;37(1):e1-2. doi: 10.1016/j.genhosppsych.2014.11.001. Epub 2014 Nov 8. Gen Hosp Psychiatry. 2015. PMID: 25467074 No abstract available.
-
Cognitive Impairment Caused by Isolated Adrenocorticotropic Hormone Deficiency without Other Hypo-adrenalism Signs - Autoimmune Encephalopathy Mimics.Intern Med. 2020 Jan 1;59(1):119-120. doi: 10.2169/internalmedicine.3234-19. Epub 2019 Jul 31. Intern Med. 2020. PMID: 31366802 Free PMC article.
-
Neurological symptoms in a patient with isolated adrenocorticotropin deficiency: case report and literature review.BMC Endocr Disord. 2016 Jan 12;16:2. doi: 10.1186/s12902-015-0082-6. BMC Endocr Disord. 2016. PMID: 26754976 Free PMC article. Review.
-
Psychiatric symptoms in a patient with isolated adrenocorticotropin deficiency: case report and literature review.Gen Hosp Psychiatry. 2014 Jul-Aug;36(4):449.e3-5. doi: 10.1016/j.genhosppsych.2014.02.012. Epub 2014 Mar 5. Gen Hosp Psychiatry. 2014. PMID: 24725972 Review.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
