

Cardiovascular Disease Prognostic Models in Latin America and the Caribbean: A Systematic Review
- PMID: 31036306
- PMCID: PMC6499414
- DOI: 10.1016/j.gheart.2019.03.001
Cardiovascular Disease Prognostic Models in Latin America and the Caribbean: A Systematic Review
Abstract
Background: Cardiovascular prognostic models guide treatment allocation and support clinical decisions. Whether there are valid models for Latin American and Caribbean (LAC) populations is unknown.
Objective: This study sought to identify and critically appraise cardiovascular prognostic models developed, tested, or recalibrated in LAC populations.
Methods: The systematic review followed the CHARMS (CHecklist for critical Appraisal and data extraction for systematic Reviews of prediction Modelling Studies) framework (PROSPERO [International Prospective Register of Systemic Reviews]: CRD42018096553). Reports were included if they followed a prospective design and presented a multivariable prognostic model; reports were excluded if they studied symptomatic individuals or patients. The following search engines were used: EMBASE, MEDLINE, Scopus, SciELO, and LILACS. Risk of bias assessment was conducted with PROBAST (Prediction model Risk Of Bias ASsessment Tool). No quantitative summary was conducted due to large heterogeneity.
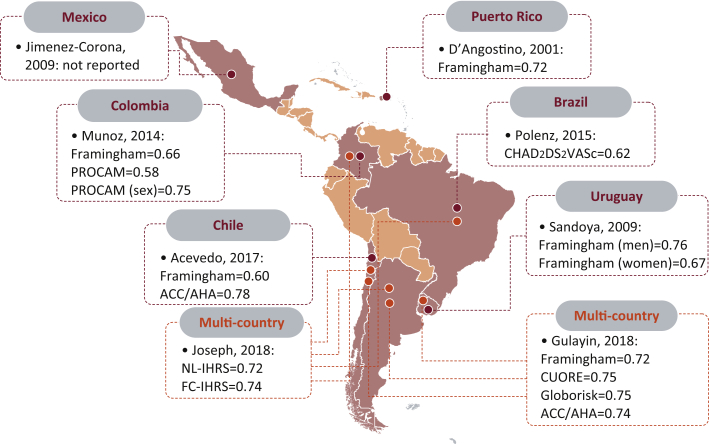
Results: From 2,506 search results, 8 studies (N = 130,482 participants) were included for qualitative synthesis. We could not identify any cardiovascular prognostic model developed for LAC populations; reviewed reports evaluated available models or conducted a recalibration analysis. Only 1 study included a Caribbean population (Puerto Rico); 3 studies were retrieved from Chile; 2 from Argentina, Brazil, Colombia, and Uruguay; and 1 from Mexico. Four studies included population-based samples, and the other 4 included people affiliated to a health facility (e.g., prevention clinics). Most studied participants were older than 50 years, and there were more women in 5 reports. The Framingham model was assessed 6 times, and the American College of Cardiology/American Heart Association pooled equation was assessed twice. Across the prognostic models assessed, calibration varied widely from one population to another, showing great overestimation particularly in some subgroups (e.g., highest risk). Discrimination (e.g., C-statistic) was acceptable for most models; for Framingham it ranged from 0.66 to 0.76. The American College of Cardiology/American Heart Association pooled equation showed the best discrimination (0.78). That there were few outcome events was the most important methodological limitation of the identified studies.
Conclusions: No cardiovascular prognostic models have been developed in LAC, hampering key evidence to inform public health and clinical practice. Validation studies need to improve methodological issues.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: a systematic review and meta-analysis.Cochrane Database Syst Rev. 2020 Jul 31;7(7):CD012022. doi: 10.1002/14651858.CD012022.pub2. Cochrane Database Syst Rev. 2020. PMID: 32735048 Free PMC article.
-
FINDRISC in Latin America: a systematic review of diagnosis and prognosis models.BMJ Open Diabetes Res Care. 2020 Apr;8(1):e001169. doi: 10.1136/bmjdrc-2019-001169. BMJ Open Diabetes Res Care. 2020. PMID: 32327446 Free PMC article.
-
[Toward a model of communications in public health in Latin America and the Caribbean].Rev Panam Salud Publica. 2005 Dec;18(6):427-38. doi: 10.1590/s1020-49892005001000006. Rev Panam Salud Publica. 2005. PMID: 16536929 Review. Spanish.
-
Nontraditional Risk Factors in Cardiovascular Disease Risk Assessment: A Systematic Evidence Report for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Jul. Report No.: 17-05225-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Jul. Report No.: 17-05225-EF-1. PMID: 30234933 Free Books & Documents. Review.
Cited by
-
Prognostic models for predicting in-hospital paediatric mortality in resource-limited countries: a systematic review.BMJ Open. 2020 Oct 19;10(10):e035045. doi: 10.1136/bmjopen-2019-035045. BMJ Open. 2020. PMID: 33077558 Free PMC article.
-
Insulin Resistance Indexes as Biomarkers of Lifetime Cardiovascular Risk among Adults from Peru.J Nutr Metab. 2021 Mar 25;2021:6633700. doi: 10.1155/2021/6633700. eCollection 2021. J Nutr Metab. 2021. PMID: 33833874 Free PMC article.
-
Prediction Models for Prognosis of Cervical Cancer: Systematic Review and Critical Appraisal.Front Public Health. 2021 May 7;9:654454. doi: 10.3389/fpubh.2021.654454. eCollection 2021. Front Public Health. 2021. PMID: 34026714 Free PMC article.
-
Epidemiology of cardiometabolic health in Latin America and strategies to address disparities.Nat Rev Cardiol. 2024 Dec;21(12):849-864. doi: 10.1038/s41569-024-01058-2. Epub 2024 Jul 25. Nat Rev Cardiol. 2024. PMID: 39054376 Free PMC article. Review.
-
Derivation, internal validation, and recalibration of a cardiovascular risk score for Latin America and the Caribbean (Globorisk-LAC): A pooled analysis of cohort studies.Lancet Reg Health Am. 2022 May;9:None. doi: 10.1016/j.lana.2022.100258. Lancet Reg Health Am. 2022. PMID: 35711683 Free PMC article.
References
-
- GBD 2016 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1260–1344. - PMC - PubMed
-
- Rose G. Sick individuals and sick populations. Int J Epidemiol. 1985;14:32–38. - PubMed
-
- Rose G. Sick individuals and sick populations. Int J Epidemiol. 2001;30:427–432. discussion 433–4. - PubMed
