

Potential for additional government spending on HIV/AIDS in 137 low-income and middle-income countries: an economic modelling study
- PMID: 31036482
- PMCID: PMC6540601
- DOI: 10.1016/S2352-3018(19)30038-4
Potential for additional government spending on HIV/AIDS in 137 low-income and middle-income countries: an economic modelling study
Abstract
Background: Between 2012 and 2016, development assistance for HIV/AIDS decreased by 20·0%; domestic financing is therefore critical to sustaining the response to HIV/AIDS. To understand whether domestic resources could fill the financing gaps created by declines in development assistance, we aimed to track spending on HIV/AIDS and estimated the potential for governments to devote additional domestic funds to HIV/AIDS.
Methods: We extracted 8589 datapoints reporting spending on HIV/AIDS. We used spatiotemporal Gaussian process regression to estimate a complete time series of spending by domestic sources (government, prepaid private, and out-of-pocket) and spending category (prevention, and care and treatment) from 2000 to 2016 for 137 low-income and middle-income countries (LMICs). Development assistance data for HIV/AIDS were from Financing Global Health 2018, and HIV/AIDS prevalence, incidence, and mortality were from the Global Burden of Disease study 2017. We used stochastic frontier analysis to estimate potential additional government spending on HIV/AIDS, which was conditional on the current government health budget and other finance, economic, and contextual factors associated with HIV/AIDS spending. All spending estimates were reported in 2018 US$.
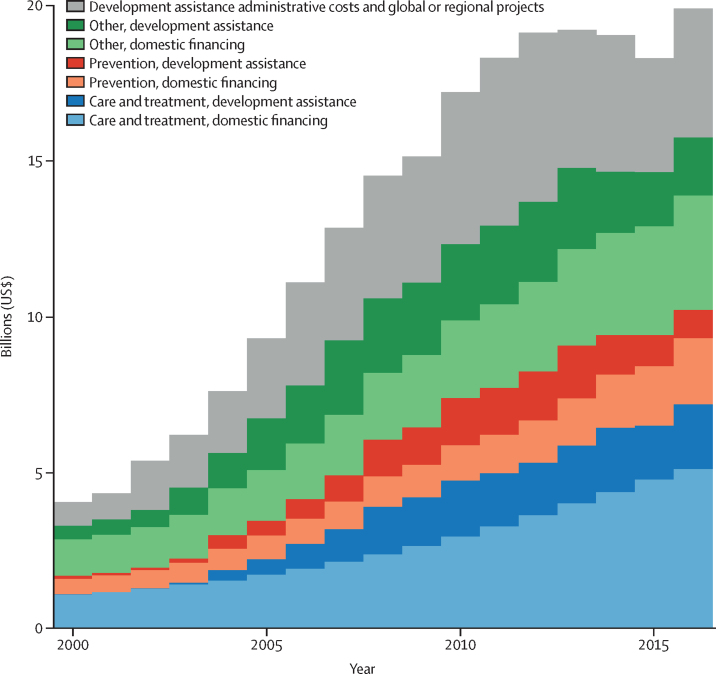
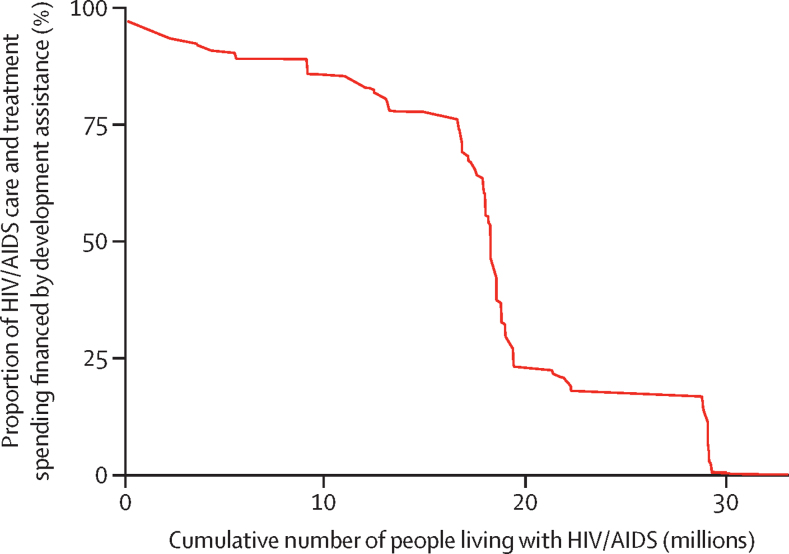
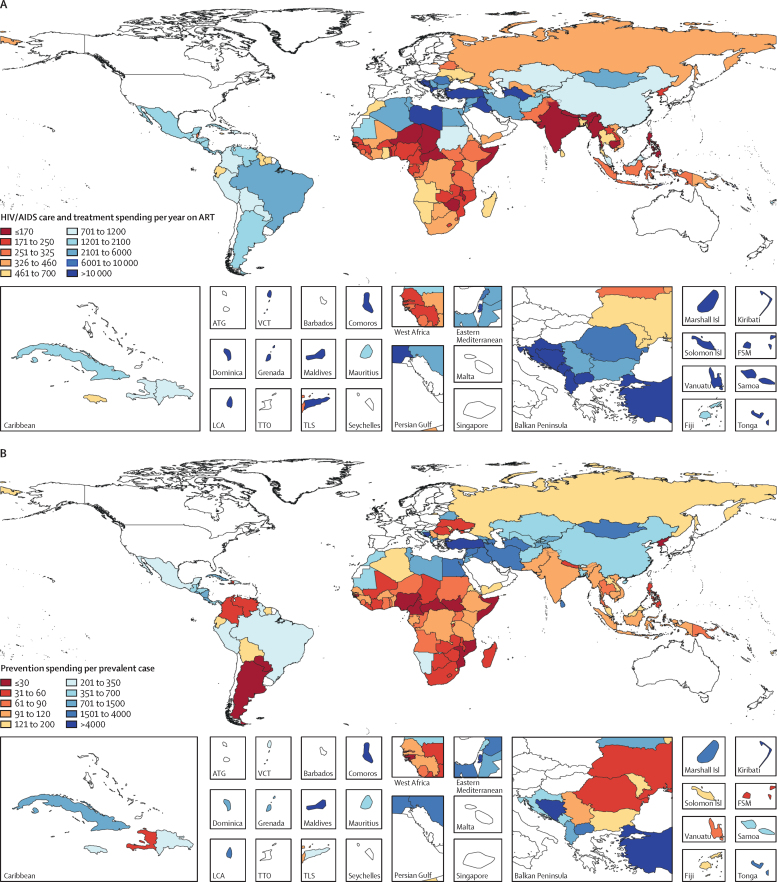
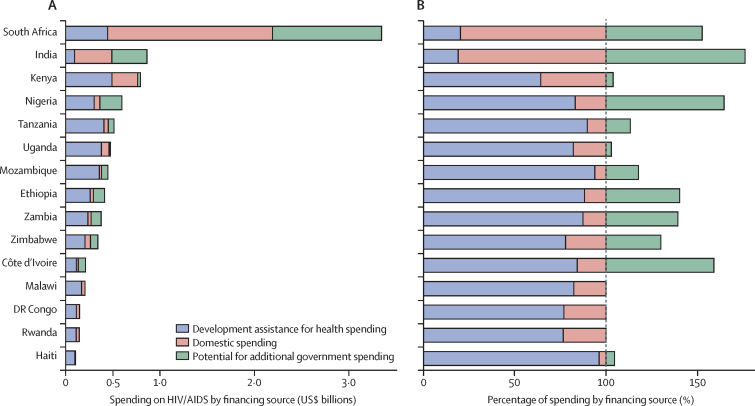
Findings: Between 2000 and 2016, total spending on HIV/AIDS in LMICs increased from $4·0 billion (95% uncertainty interval 2·9-6·0) to $19·9 billion (15·8-26·3), spending on HIV/AIDS prevention increased from $596 million (258 million to 1·3 billion) to $3·0 billion (1·5-5·8), and spending on HIV/AIDS care and treatment increased from $1·1 billion (458·1 million to 2·2 billion) to $7·2 billion (4·3-11·8). Over this time period, the share of resources sourced from development assistance increased from 33·2% (21·3-45·0) to 46·0% (34·2-57·0). Care and treatment spending per year on antiretroviral therapy varied across countries, with an IQR of $284-2915. An additional $12·1 billion (8·4-17·5) globally could be mobilised by governments of LMICs to finance the response to HIV/AIDS. Most of these potential resources are concentrated in ten middle-income countries (Argentina, China, Colombia, India, Indonesia, Mexico, Nigeria, Russia, South Africa, and Vietnam).
Interpretation: Some governments could mobilise more domestic resources to fight HIV/AIDS, which could free up additional development assistance for many countries without this ability, including many low-income, high-prevalence countries. However, a large gap exists between available financing and the funding needed to achieve global HIV/AIDS goals, and sustained and coordinated effort across international and domestic development partners is required to end AIDS by 2030.
Funding: The Bill & Melinda Gates Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Estimating fiscal space for health: pitfalls and solutions.Lancet HIV. 2019 Jun;6(6):e345-e346. doi: 10.1016/S2352-3018(19)30131-6. Epub 2019 Apr 25. Lancet HIV. 2019. PMID: 31031183 No abstract available.
References
-
- Dicker D, Nguyen G, Abate D. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1684–1735. - PMC - PubMed
- D Dicker, G Nguyen, D Abate. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet, 392, 2018, 1684–1735 - PMC - PubMed
-
- James SL, Abate D, Abate KH. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. - PMC - PubMed
- SL James, D Abate, KH Abate. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet, 392, 2018, 1789–1858 - PMC - PubMed
-
- Stover J, Bollinger L, Izazola JA. What is required to end the AIDS epidemic as a public health threat by 2030? The cost and impact of the fast-track approach. PLoS One. 2016;11:e0154893. - PMC - PubMed
- J Stover, L Bollinger, JA Izazola. What is required to end the AIDS epidemic as a public health threat by 2030? The cost and impact of the fast-track approach. PLoS One, 11, 2016, e0154893 - PMC - PubMed
-
- UNAIDS 90-90-90: An ambitious treatment target to help end the AIDS epidemic. October, 2014. http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
- UNAID, S 90-90-90: An ambitious treatment target to help end the AIDS epidemic, http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pd, ctober, 2014
-
- Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet. 2009;373:48–57. - PubMed
- RM Granich, CF Gilks, C Dye, KM De Cock, BG Williams. Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet, 373, 2009, 48–57 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
