

Corticospinal Tract Integrity and Long-Term Hand Function Prognosis in Patients With Stroke
- PMID: 31037066
- PMCID: PMC6476282
- DOI: 10.3389/fneur.2019.00374
Corticospinal Tract Integrity and Long-Term Hand Function Prognosis in Patients With Stroke
Abstract
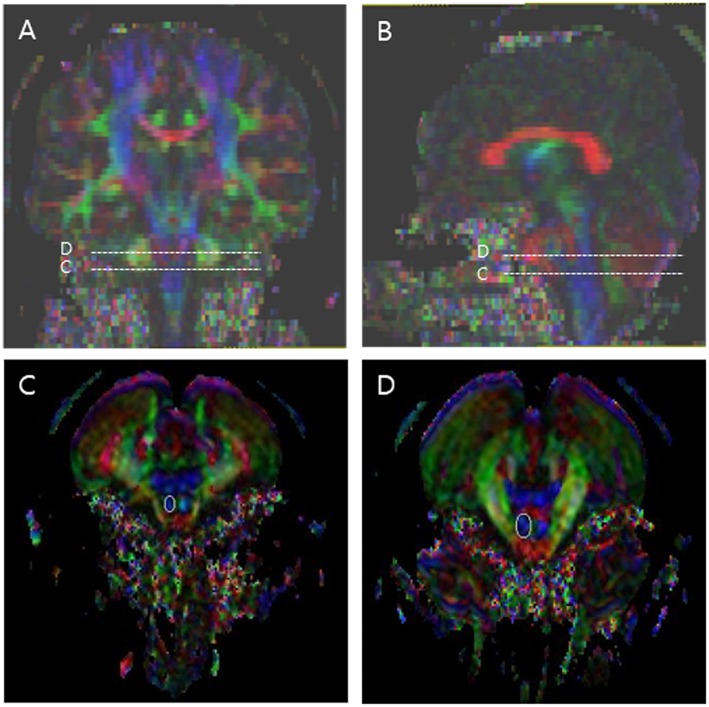
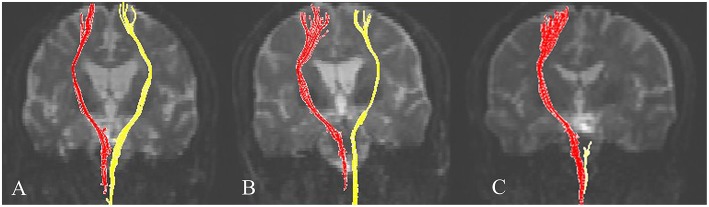
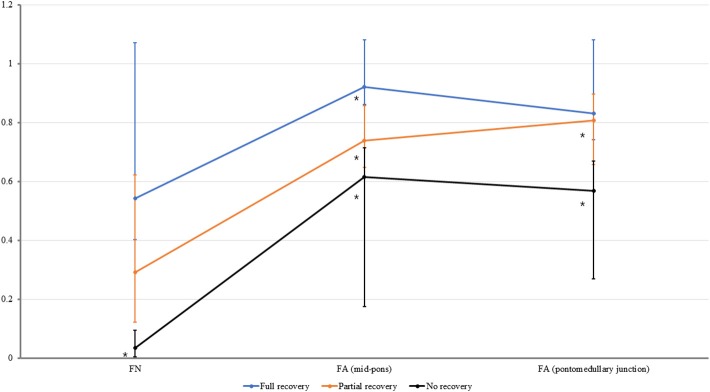
Background: The restoration of hand function is an important goal for patients with stroke. This study investigated the relationship between corticospinal tract (CST) integrity and the functional status of the hand in patients with stroke 6 months after onset and evaluated which of the following values would be useful for predicting hand function: fiber number (FN), fractional anisotropy (FA) at the mid-pons, and FA at the pontomedullary junction. Methods: The present retrospective cross-sectional observational study assessed 44 patients with stroke who were able to walk without using a walking aid or orthosis. The final hand function results were classified into three groups: no recovery (unable to grasp), partial recovery (able to grasp, unable to oppose), and full recovery (able to grasp and oppose). All subjects underwent diffusion tensor imaging (DTI) at 6 months after stroke onset. Values for FA at the mid-pons and pontomedullary junction and CST FN were measured. The normalization ratio for FN and FA was calculated using the following formula: data for affected hand/data for non-affected hand. Results: The normalized FN, FA (mid-pons), and FA (pontomedullary junction) DTI values differed significantly. The FA (mid-pons) value for the full recovery group was higher than those for the other groups. The FA (mid-pons) value for the partial recovery group was higher than that for the no recovery group. The normalized FA (mid-pons) value differed significantly among all three groups. Conclusions: The present study showed that CST integrity (at 6 months after onset) in patients with chronic stroke was related to functional hand status. In addition, the mid-pons FA value was more predictive of functional restoration of the hand than the FN or FA value at the pontomedullary junction. These results may be useful in predicting the functional restoration of the hand and understanding the functional prognosis of stroke.
Keywords: corticospinal tract; diffusion tensor imaging; hand function; prognosis; stroke; stroke rehabilitation.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous