

Schwannomatosis of the Spinal Accessory Nerve: A Case Report
- PMID: 31037098
- PMCID: PMC6486389
- DOI: 10.1055/s-0039-1685457
Schwannomatosis of the Spinal Accessory Nerve: A Case Report
Abstract
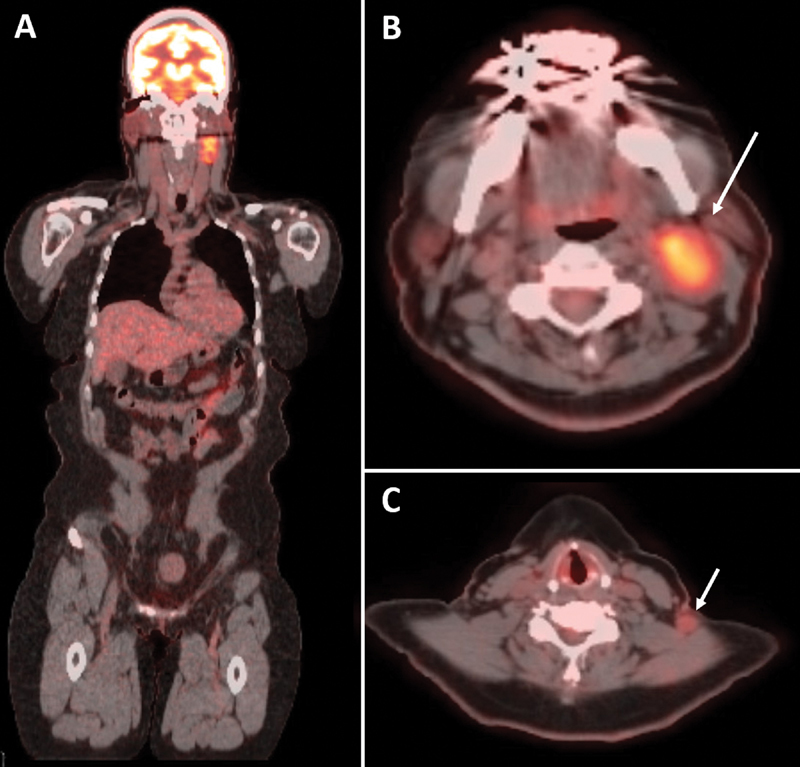
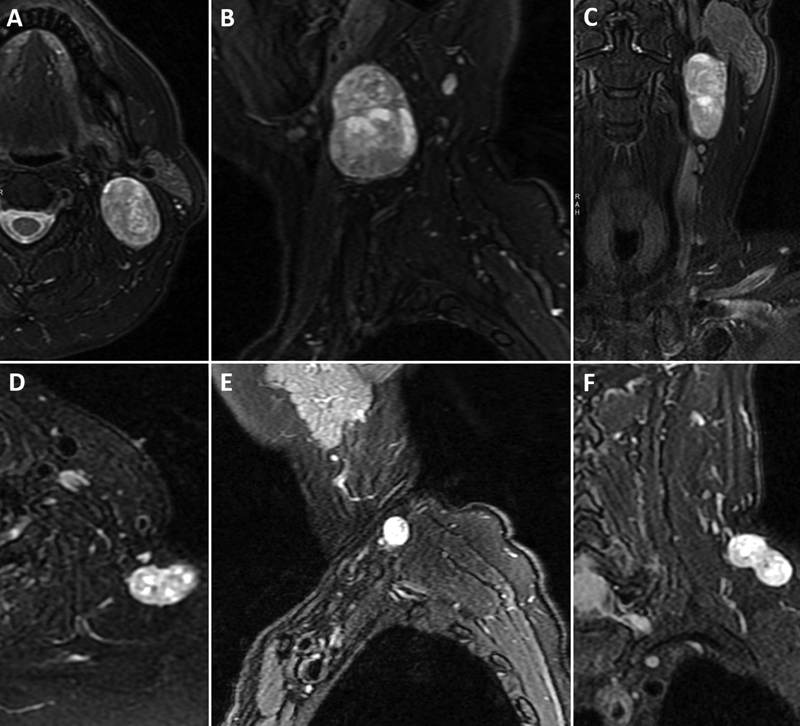
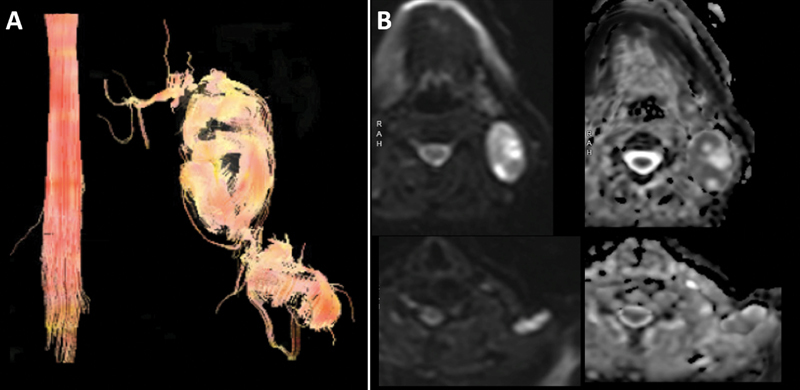
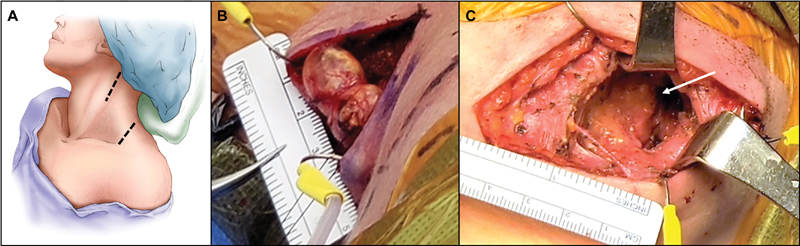
Schwannomatosis is a distinct syndrome characterized by multiple peripheral nerve schwannomas that can be sporadic or familial in nature. Cases affecting the lower cranial nerves are infrequent. Here, the authors present a rare case of schwannomatosis affecting the left spinal accessory nerve. Upon genetic screening, an in-frame insertion at codon p.R177 of the Sox 10 gene was observed. There were no identifiable alterations in NF1, NF2, LZTR1, and SMARCB1. This case demonstrates a rare clinical presentation of schwannomatosis in addition to a genetic aberration that has not been previously reported in this disease context.
Keywords: diffusion tensor imaging; neck mass; schwannoma; schwannomatosis; spinal accessory nerve tumor.
Conflict of interest statement
Figures
Similar articles
-
A mosaic pattern of INI1/SMARCB1 protein expression distinguishes Schwannomatosis and NF2-associated peripheral schwannomas from solitary peripheral schwannomas and NF2-associated vestibular schwannomas.Childs Nerv Syst. 2017 Jun;33(6):933-940. doi: 10.1007/s00381-017-3340-2. Epub 2017 Apr 1. Childs Nerv Syst. 2017. PMID: 28365909
-
Schwannomatosis: a genetic and epidemiological study.J Neurol Neurosurg Psychiatry. 2018 Nov;89(11):1215-1219. doi: 10.1136/jnnp-2018-318538. Epub 2018 Jun 16. J Neurol Neurosurg Psychiatry. 2018. PMID: 29909380
-
Intraosseous schwannoma of the mandible and schwannoma of the spinal cord: A rare presentation of schwannomatosis - Case report and review of the literature.Natl J Maxillofac Surg. 2019 Jul-Dec;10(2):267-269. doi: 10.4103/njms.NJMS_49_16. Epub 2019 Nov 12. Natl J Maxillofac Surg. 2019. PMID: 31798271 Free PMC article.
-
The molecular pathogenesis of schwannomatosis, a paradigm for the co-involvement of multiple tumour suppressor genes in tumorigenesis.Hum Genet. 2017 Feb;136(2):129-148. doi: 10.1007/s00439-016-1753-8. Epub 2016 Dec 5. Hum Genet. 2017. PMID: 27921248 Free PMC article. Review.
-
Cancer and Central Nervous System Tumor Surveillance in Pediatric Neurofibromatosis 2 and Related Disorders.Clin Cancer Res. 2017 Jun 15;23(12):e54-e61. doi: 10.1158/1078-0432.CCR-17-0590. Clin Cancer Res. 2017. PMID: 28620005 Review.
Cited by
-
Managing Multiple Schwannomatosis of Vagus and Hypoglossal Nerves: The Unanticipated Complications.Indian J Otolaryngol Head Neck Surg. 2023 Jun;75(2):1162-1168. doi: 10.1007/s12070-022-03460-z. Epub 2023 Jan 6. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37275115 Free PMC article.
-
Hereditary intraspinal schwannomatosis with SMARCB1 gene mutation: A case report.J Clin Lab Anal. 2022 Jun;36(6):e24448. doi: 10.1002/jcla.24448. Epub 2022 Apr 21. J Clin Lab Anal. 2022. PMID: 35446994 Free PMC article.
-
Clinical Effect of Laminectomy with Lateral Mass Screw Fixation in Treating Cervical Schwannoma: A Retrospective Study.Biomed Res Int. 2022 Apr 29;2022:8512374. doi: 10.1155/2022/8512374. eCollection 2022. Biomed Res Int. 2022. PMID: 35528181 Free PMC article.
References
-
- International Agency for Research on Cancer.WHO Classification of Tumors of the Central Nervous System. 4th ed Geneva: World Health Organization; 2016
-
- MacCollin M, Chiocca E A, Evans D G et al.Diagnostic criteria for schwannomatosis. Neurology. 2005;64(11):1838–1845. - PubMed
-
- Evans D G, Bowers N L, Tobi S et al.Schwannomatosis: a genetic and epidemiological study. J Neurol Neurosurg Psychiatry. 2018;89(11):1215–1219. - PubMed
-
- Huang J H, Simon S L, Nagpal S, Nelson P T, Zager E L.Management of patients with schwannomatosis: report of six cases and review of the literature Surg Neurol 20046204353–361., discussion 361 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous