

HER2-Enriched Subtype and ERBB2 Expression in HER2-Positive Breast Cancer Treated with Dual HER2 Blockade
- PMID: 31037288
- PMCID: PMC7850037
- DOI: 10.1093/jnci/djz042
HER2-Enriched Subtype and ERBB2 Expression in HER2-Positive Breast Cancer Treated with Dual HER2 Blockade
Abstract
Background: Identification of HER2-positive breast cancers with high anti-HER2 sensitivity could help de-escalate chemotherapy. Here, we tested a clinically applicable RNA-based assay that combines ERBB2 and the HER2-enriched (HER2-E) intrinsic subtype in HER2-positive disease treated with dual HER2-blockade without chemotherapy.
Methods: A research-based PAM50 assay was applied in 422 HER2-positive tumors from five II-III clinical trials (SOLTI-PAMELA, TBCRC023, TBCRC006, PER-ELISA, EGF104090). In SOLTI-PAMELA, TBCRC023, TBCRC006, and PER-ELISA, all patients had early disease and were treated with neoadjuvant lapatinib or pertuzumab plus trastuzumab for 12-24 weeks. Primary outcome was pathological complete response (pCR). In EGF104900, 296 women with advanced disease were randomized to receive either lapatinib alone or lapatinib plus trastuzumab. Progression-free survival (PFS), overall response rate (ORR), and overall survival (OS) were evaluated.
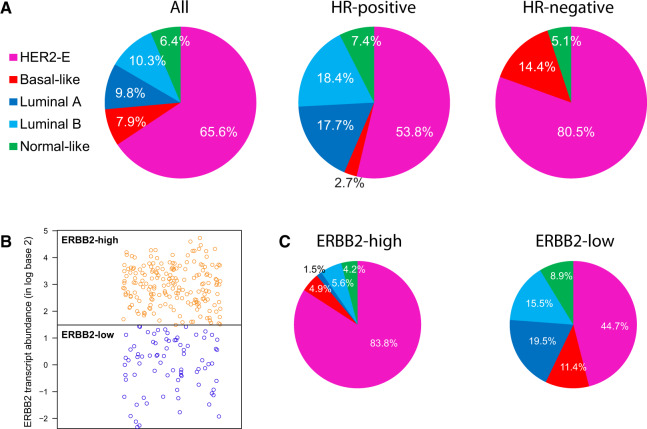
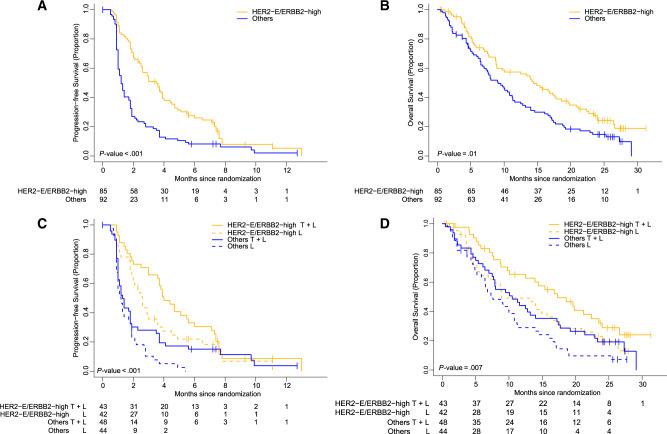
Results: A total of 305 patients with early and 117 patients with advanced HER2-positive disease were analyzed. In early disease, HER2-E represented 83.8% and 44.7% of ERBB2-high and ERBB2-low tumors, respectively. Following lapatinib and trastuzumab, the HER2-E and ERBB2 (HER2-E/ERBB2)-high group showed a higher pCR rate compared to the rest (44.5%, 95% confidence interval [CI] = 35.4% to 53.9% vs 11.6%, 95% CI = 6.9% to 18.0%; adjusted odds ratio [OR] = 6.05, 95% CI = 3.10 to 11.80, P < .001). Similar findings were observed with neoadjuvant trastuzumab and pertuzumab (pCR rate of 66.7% in HER2-E/ERBB2-high, 95% CI = 22.3% to 95.7% vs 14.7% in others, 95% CI = 4.9% to 31.1%; adjusted OR = 11.60, 95% CI = 1.66 to 81.10, P = .01). In the advanced setting, the HER2-E/ERBB2-high group was independently associated with longer PFS (hazard ratio [HR] = 0.52, 95% CI = 0.35 to 0.79, P < .001); higher ORR (16.3%, 95% CI = 8.9% to 26.2% vs 3.7%, 95% CI = 0.8% to 10.3%, P = .02); and longer OS (HR = 0.66, 95% CI = 0.44 to 0.97, P = .01).
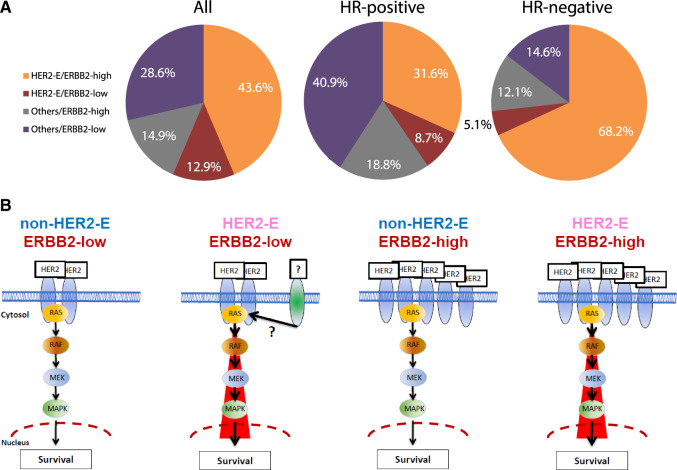
Conclusions: Combining HER2-E subtype and ERBB2 mRNA into a single assay identifies tumors with high responsiveness to HER2-targeted therapy. This biomarker could help de-escalate chemotherapy in approximately 40% of patients with HER2-positive breast cancer.
© The Author(s) 2019. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Blackwell KL, Burstein HJ, Storniolo AM, et al. Overall survival benefit with lapatinib in combination with trastuzumab for patients with human epidermal growth factor receptor 2–positive metastatic breast cancer: final results from the EGF104900 study. J Clinc Oncol. 2012;30(21):2585–2592. - PubMed
-
- Rimawi MF, Mayer IA, Forero A, et al. Multicenter phase II study of neoadjuvant lapatinib and trastuzumab with hormonal therapy and without chemotherapy in patients with human epidermal growth factor receptor 2–overexpressing breast cancer: TBCRC 006. J Clinc Oncol. 2013;31(14):1726–1731. - PMC - PubMed
-
- Rimawi MF, Niravath PA, Wang T, et al. Abstract S6-02: TBCRC023: a randomized multicenter phase II neoadjuvant trial of lapatinib plus trastuzumab, with endocrine therapy and without chemotherapy, for 12 vs. 24 weeks in patients with HER2 overexpressing breast cancer. Cancer Res. 2015;75(suppl 9):S6-02-S6-02. - PubMed
-
- Llombart-Cussac A, Cortés J, Paré L, et al. HER2-enriched subtype as a predictor of pathological complete response following trastuzumab and lapatinib without chemotherapy in early-stage HER2-positive breast cancer (PAMELA): an open-label, single-group, multicentre, phase 2 trial. Lancet Oncol. 2017;18(4):545–554. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
