

RACHS - ANZ : A Modified Risk Adjustment in Congenital Heart Surgery Model for Outcome Surveillance in Australia and New Zealand
- PMID: 31039662
- PMCID: PMC6512128
- DOI: 10.1161/JAHA.118.011390
RACHS - ANZ : A Modified Risk Adjustment in Congenital Heart Surgery Model for Outcome Surveillance in Australia and New Zealand
Abstract
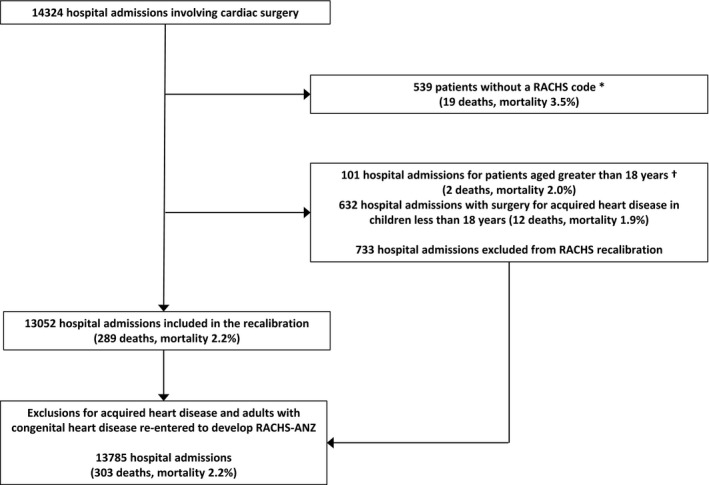
Background Outcomes for pediatric cardiac surgery are commonly reported from international databases compiled from voluntary data submissions. Surgical outcomes for all children in a country or region are less commonly reported. We aimed to describe the bi-national population-based outcome for children undergoing cardiac surgery in Australia and New Zealand and determine whether the Risk Adjustment for Congenital Heart Surgery ( RACHS ) classification could be used to create a model that accurately predicts in-hospital mortality in this population. Methods and Results The study was conducted in all children's hospitals performing cardiac surgery in Australia and New Zealand between January 2007 and December 2015. The performance of the original RACHS -1 model was assessed and compared with an alternative RACHS - ANZ (Australia and New Zealand) model, developed balancing discrimination with parsimonious variable selection. A total of 14 324 hospital admissions were analyzed. The overall hospital mortality was 2.3%, ranging from 0.5% for RACHS category 1 procedures, to 17.0% for RACHS category 5 or 6 procedures. The original RACHS -1 model was poorly calibrated with death overpredicted (1161 deaths predicted, 289 deaths observed). The RACHS - ANZ model had better performance in this population with excellent discrimination (Az- ROC of 0.830) and acceptable Hosmer and Lemeshow goodness-of-fit ( P=0.216). Conclusions The original RACHS -1 model overpredicts mortality in children undergoing heart surgery in the current era. The RACHS - ANZ model requires only 3 risk variables in addition to the RACHS procedure category, can be applied to a wider range of patients than RACHS -1, and is suitable to use to monitor regional pediatric cardiac surgery outcomes.
Keywords: cardiac surgery; congenital heart disease; outcome and process assessment; pediatric; risk model.
Figures
References
-
- van der Bom T, Zomer AC, Zwinderman AH, Meijboom FJ, Bouma BJ, Mulder BJM. The changing epidemiology of congenital heart disease. Nat Rev Cardiol. 2011;8:50–60. - PubMed
-
- Lacour‐Gayet F, Clarke D, Jacobs J, Comas J, Daebritz S, Daenen W, Gaynor W, Hamilton L, Jacobs M, Maruszsewski B, Pozzi M, Spray T, Stellin G, Tchervenkov C, Mavroudis C. The Aristotle score: a complexity‐adjusted method to evaluate surgical results. Eur J Cardiothorac Surg. 2004;25:911–924. - PubMed
-
- Jenkins KJ, Gauvreau K, Newburger JW, Spray TL, Moller JH, Iezzoni LI. Consensus‐based method for risk adjustment for surgery for congenital heart disease. J Thorac Cardiovasc Surg. 2002;123:110–118. - PubMed
-
- O'Brien SM, Clarke DR, Jacobs JP, Jacobs ML, Lacour‐Gayet FG, Pizarro C, Welke KF, Maruszewski B, Tobota Z, Miller WJ, Hamilton L, Peterson ED, Mavroudis C, Edwards FH. An empirically based tool for analyzing mortality associated with congenital heart surgery. J Thorac Cardiovasc Surg. 2009;138:1139–1153. - PubMed
-
- Straney L, Clements A, Parslow RC, Pearson G, Shann F, Alexander J, Slater A. Paediatric Index of Mortality 3: an updated model for predicting mortality in pediatric intensive care. Pediatr Crit Care Med. 2013;14:673–681. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
