

Use of antidepressants and anxiolytics in early pregnancy and the risk of preeclampsia and gestational hypertension: a prospective study
- PMID: 31039756
- PMCID: PMC6492434
- DOI: 10.1186/s12884-019-2285-8
Use of antidepressants and anxiolytics in early pregnancy and the risk of preeclampsia and gestational hypertension: a prospective study
Abstract
Background: We investigated the association between antidepressant and anxiolytic exposure during the first and early second trimester of pregnancy (< 16 weeks), and hypertensive disorders of pregnancy (including preeclampsia and gestational hypertension) in women with singleton pregnancy.
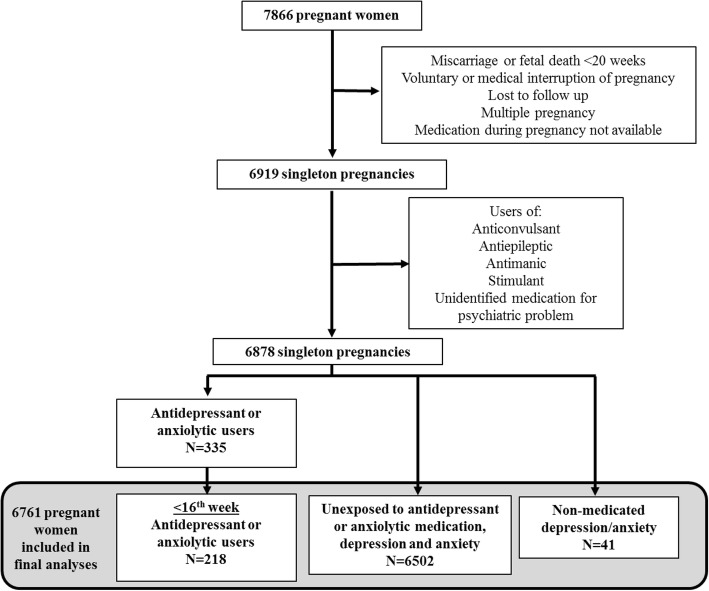
Methods: This study is based on a large prospective cohort of 7866 pregnant women. We included pregnant women aged 18 years or older without chronic hepatic or renal disease at the time of recruitment. Participants lost to the follow-up, with multiple pregnancies and pregnancy terminations, miscarriages or fetal deaths before 20 weeks of gestation were excluded from the study, as well as women with no data on the antidepressant/anxiolytic medication use during pregnancy. Information concerning antidepressant or anxiolytic medication use was extracted from hospital records after delivery. The associations between their use and the risk of gestational hypertension or preeclampsia were calculated.
Results: The final sample for analysis included 6761 participants including 218 (3.2%) women who were exposed to antidepressant and/or anxiolytic medication before the 16th week of gestation. Forty-one women had a non-medicated depression or anxiety during the pregnancy. Moreover, 195 (2.9%) and 122 (1.8%) women developed gestational hypertension and preeclampsia respectively. When compared to women unexposed to antidepressant/anxiolytic medication, depression and anxiety, those using antidepressant and/or anxiolytic drugs before the 16th week of gestation were at increased risk of preeclampsia (adjusted odd ratio (aOR) 3.09 [CI95% 1.56-6.12]), especially if they continued their medication after the 16th week (aOR 3.41 [CI95% 1.66-7.02]) compared to those who did not (1.60 [CI95% 0.21-12.34]).
Conclusions: Women exposed to antidepressant and/or anxiolytic medication before the 16th week of pregnancy have a 3-fold increased risk for preeclampsia when compared to women unexposed to antidepressant/anxiolytic medication, depression and anxiety. Also, our results suggested that women who stopped their medication before the 16th week of pregnancy could be benefit from reduced preeclampsia risk.
Keywords: Antidepressants; Anxiolytics; Pregnancy; Risk of preeclampsia; women’s health.
Conflict of interest statement
Ethics approval and consent to participate
Participants gave written informed consent to participate to a large prospective cohort on pregnancy complications and birth outcomes (Human biological specimen bank for the study of complications of pregnancy, maternal-fetal exchanges and their subsequent consequences). This current study was approved by the CHU de Québec-Université Laval Ethics Review Board (initial approval date: 9 November 2004, Project 5–04–10-01 [95.05.17 l SC12–01-159).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
