

Validated model for prediction of recurrent hepatocellular carcinoma after liver transplantation in Asian population
- PMID: 31040897
- PMCID: PMC6475674
- DOI: 10.4251/wjgo.v11.i4.322
Validated model for prediction of recurrent hepatocellular carcinoma after liver transplantation in Asian population
Abstract
Background: Liver transplantation (LT) is regarded as the best treatment for both primary and recurrent hepatocellular carcinoma (HCC). Post-transplant HCC recurrence rate is relatively low but significant, ranging from 10%-30% according to different series. When recurrence happens, it is usually extrahepatic and associated with poor prognosis. A predictive model that allows patient stratification according to recurrence risk can help to individualize post-transplant surveillance protocol and guidance of the use of anti-tumor immunosuppressive agents.
Aim: To develop a scoring system to predict HCC recurrence after LT in an Asian population.
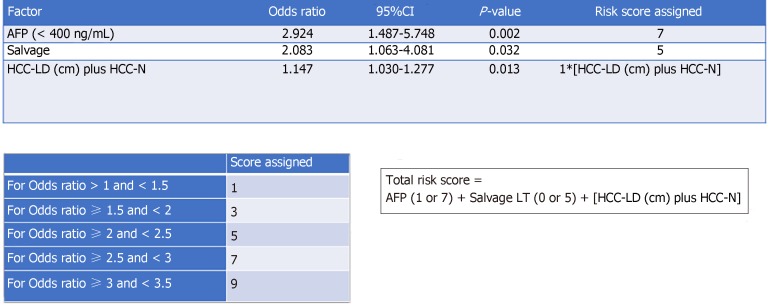
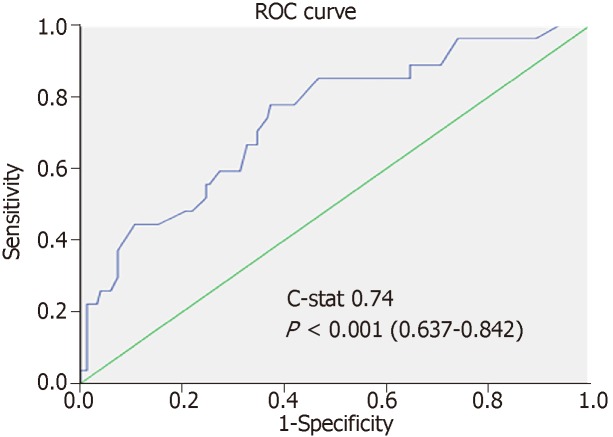
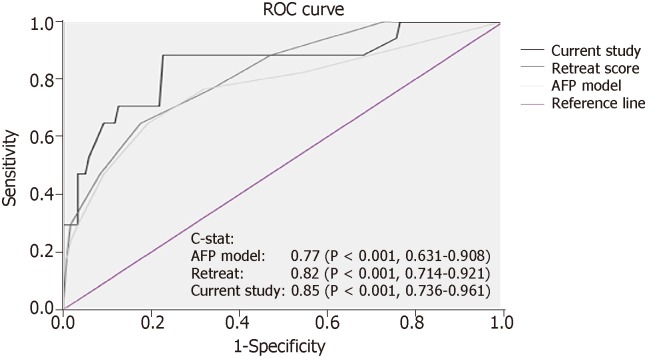
Methods: Consecutive patients having LT for HCC from 1995 to 2016 at our hospital were recruited. They were randomized into the training set and the validation set in a 60:40 ratio. Multivariable Cox regression model was used to identity factors associated with HCC recurrence. A risk score was assigned to each factor according to the odds ratio. Accuracy of the score was assessed by the area under the receiver operating characteristic curve.
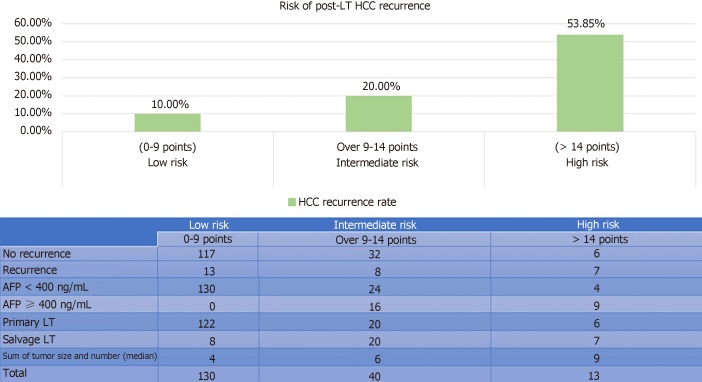
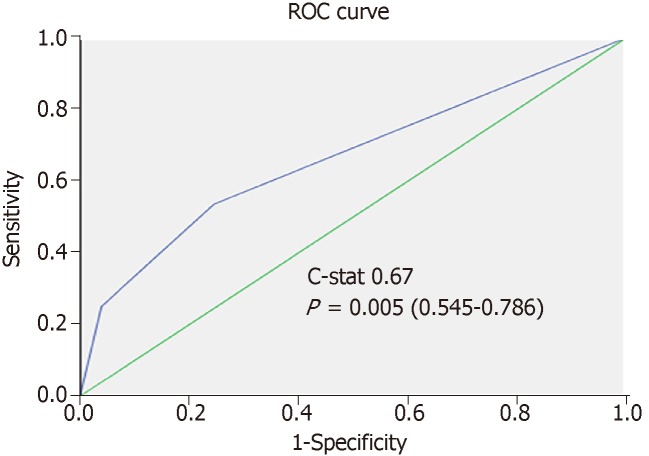
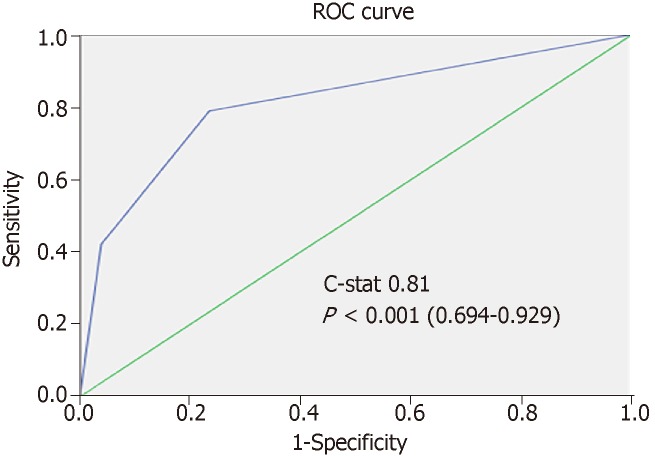
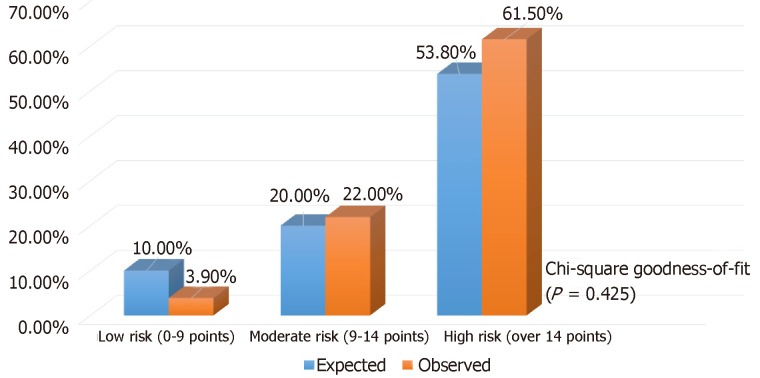
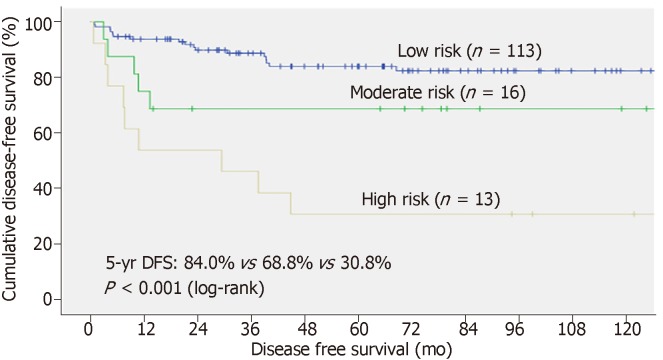
Results: In total, 330 patients were eligible for analysis (183 in training and 147 in validation). Recurrent HCC developed in 14.2% of them. The median follow-up duration was 65.6 mo. The 5-year disease-free and overall survival rates were 78% and 80%, respectively. On multivariate analysis, alpha-fetoprotein > 400 ng/mL [P = 0.012, hazard ratio (HR) 2.92], sum of maximum tumor size and number (P = 0.013, HR 1.15), and salvage LT (P = 0.033, HR 2.08) were found to be independent factors for disease-free survival. A risk score was calculated for each patient with good discriminatory power (c-stat 0.748 and 0.85, respectively, in the training and validation sets). With the derived scores, patients were classified into low- (0-9), moderate- (> 9-14), and high-risk groups (> 14), and the risk of HCC recurrence in the training and validation sets was 10%, 20%, 54% (c-stat 0.67) and 4%, 22%, 62% (c-stat 0.811), accordingly. The risk stratification model was validated with chi-squared goodness-of-fit test (P = 0.425).
Conclusion: A validated predictive model featuring alpha-fetoprotein, salvage LT, and the sum of largest tumor diameter and total number of tumor nodule provides simple and reliable guidance for individualizing postoperative surveillance strategy.
Keywords: Hepatocellular carcinoma; Liver transplantation; Post-transplant recurrence; Predictive model.
Conflict of interest statement
Conflict-of-interest statement: None of the authors has any conflict of interest.
Figures

References
-
- Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394–1403. - PubMed
-
- Nörthen A, Asendorf T, Walson PD, Oellerich M. Diagnostic value of alpha-1-fetoprotein (AFP) as a biomarker for hepatocellular carcinoma recurrence after liver transplantation. Clin Biochem. 2018;52:20–25. - PubMed
-
- Furukawa H, Shimamura T, Suzuki T, Taniguchi M, Nakanishi K, Yamashita K, Kamiyama T, Matsushita M, Todo S. Liver transplantation for hepatocellular carcinoma: the Japanese experience. J Hepatobiliary Pancreat Sci. 2010;17:533–538. - PubMed
-
- Agopian VG, Harlander-Locke M, Zarrinpar A, Kaldas FM, Farmer DG, Yersiz H, Finn RS, Tong M, Hiatt JR, Busuttil RW. A novel prognostic nomogram accurately predicts hepatocellular carcinoma recurrence after liver transplantation: analysis of 865 consecutive liver transplant recipients. J Am Coll Surg. 2015;220:416–427. - PubMed
-
- Gouw AS, Balabaud C, Kusano H, Todo S, Ichida T, Kojiro M. Markers for microvascular invasion in hepatocellular carcinoma: where do we stand? Liver Transpl. 2011;17 Suppl 2:S72–S80. - PubMed
LinkOut - more resources
Full Text Sources
