

Clinical validation of the tempus xT next-generation targeted oncology sequencing assay
- PMID: 31040929
- PMCID: PMC6481324
- DOI: 10.18632/oncotarget.26797
Clinical validation of the tempus xT next-generation targeted oncology sequencing assay
Abstract
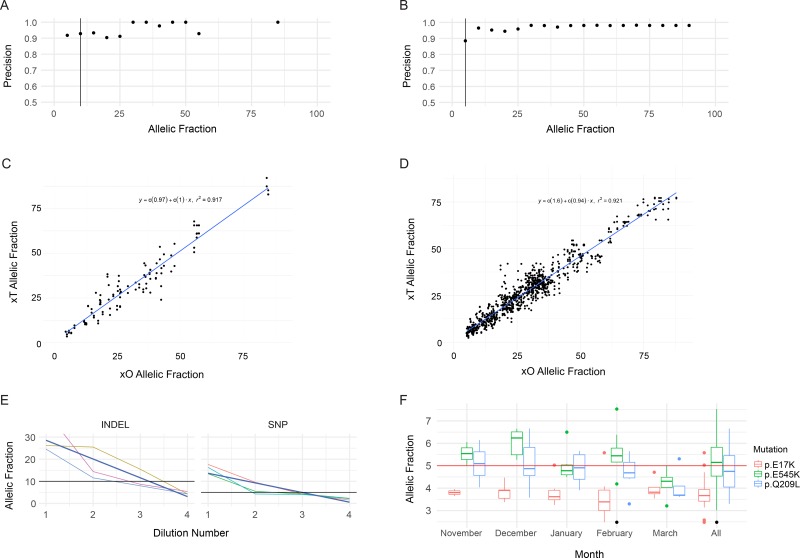
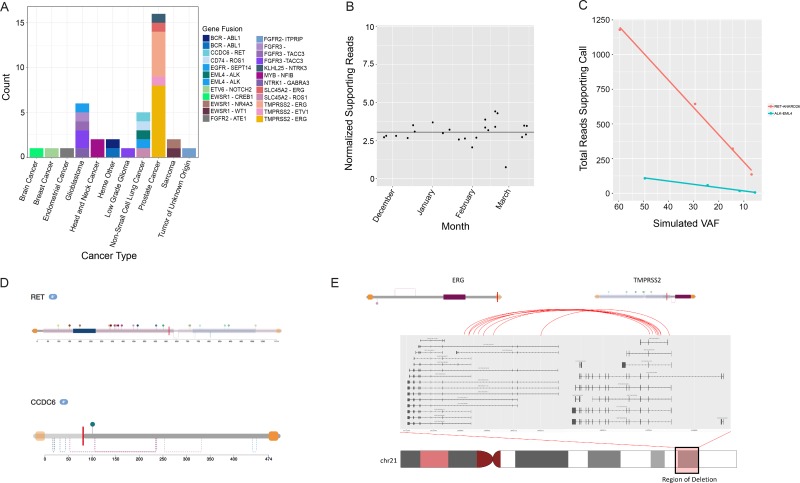
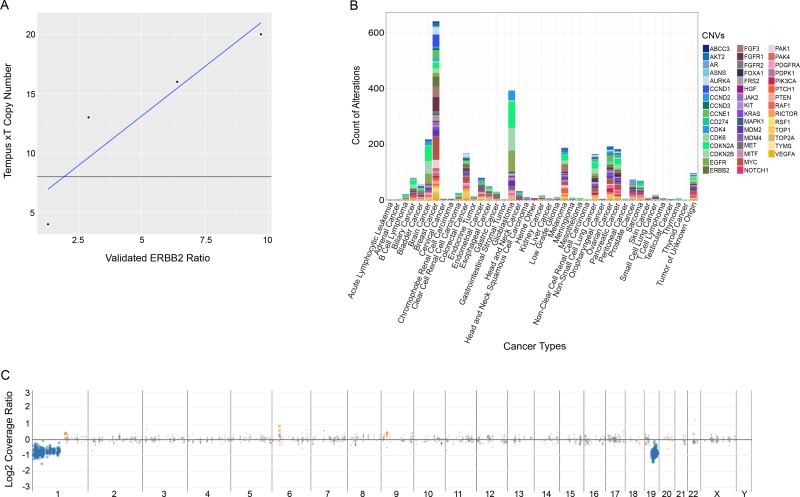
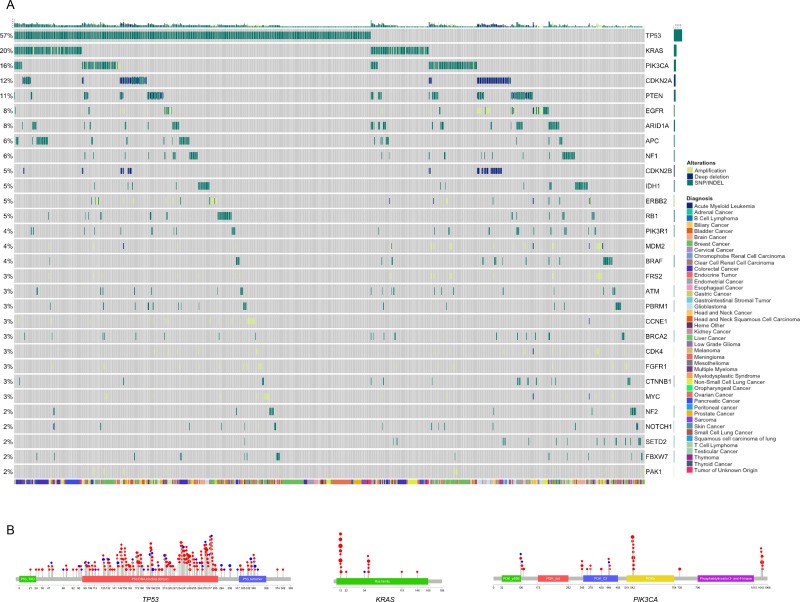
We developed and clinically validated a hybrid capture next generation sequencing assay to detect somatic alterations and microsatellite instability in solid tumors and hematologic malignancies. This targeted oncology assay utilizes tumor-normal matched samples for highly accurate somatic alteration calling and whole transcriptome RNA sequencing for unbiased identification of gene fusion events. The assay was validated with a combination of clinical specimens and cell lines, and recorded a sensitivity of 99.1% for single nucleotide variants, 98.1% for indels, 99.9% for gene rearrangements, 98.4% for copy number variations, and 99.9% for microsatellite instability detection. This assay presents a wide array of data for clinical management and clinical trial enrollment while conserving limited tissue.
Keywords: next-generation sequencing assay validation; tumor profiling.
Conflict of interest statement
CONFLICTS OF INTEREST All authors have a financial relationship as employees of Tempus Labs, Inc.
Figures

References
-
- Motzer RJ, Tannir NM, McDermott DF, Arén Frontera O, Melichar B, Choueiri TK, Plimack ER, Barthélémy P, Porta C, George S, Powles T, Donskov F, Neiman V, et al. CheckMate 214 Investigators Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. 2018;378:1277–1290. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
