

Clinicolaboratory profile of expanded dengue syndrome - Our experience in a teaching hospital
- PMID: 31041245
- PMCID: PMC6482768
- DOI: 10.4103/jfmpc.jfmpc_12_19
Clinicolaboratory profile of expanded dengue syndrome - Our experience in a teaching hospital
Abstract
Introduction: Classic dengue fever presentation has expanded its horizon by involving various organ systems and is named as expanded dengue syndrome. This changing presentation and rising burden across the globe may lead to delayed diagnosis and under reporting of this syndrome.
Aim of study: To analyze clinicolaboratory profile of patients with expanded dengue syndrome.
Materials and methods: About 520 cases of expanded dengue syndrome as per World Health Organization definition criteria 2012 were studied with their informed consent. Detailed history, thorough clinical examination, and relevant investigations were done. Their clinical and laboratory parameters were analyzed. Standard treatment guidelines were followed in all cases.
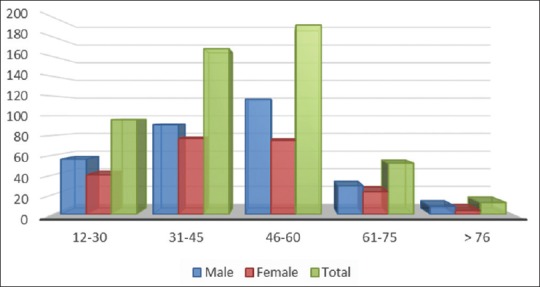
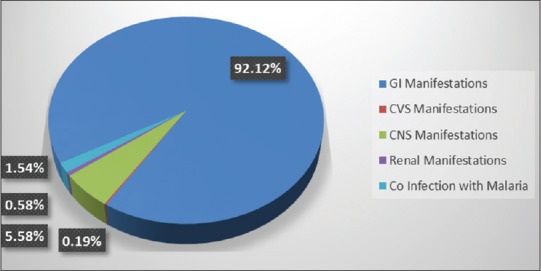
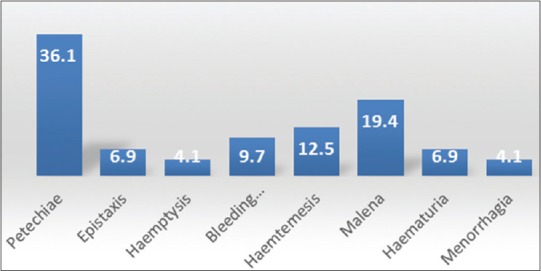
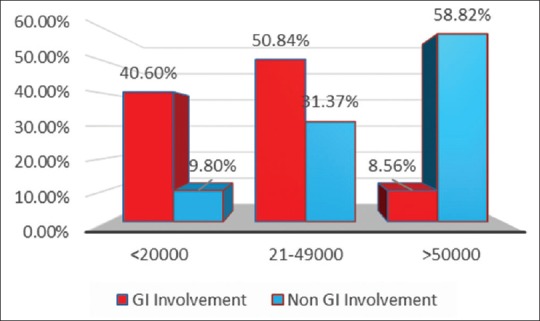
Observation: About 301 patients were male and 219 were female with male-to-female ratio of 3:2. Their age varied from 12 to 76 years with the average age of 47.5 years. About 92% of cases presented with various gastro hepatic manifestations. The commonest gastrohepatic manifestation was transaminitis (57.5%) that is asymptomatic elevation of liver enzymes followed by acalculous cholecystitis (21%) and acute pancreatitis (13.9%). Twenty-nine patients presented with various neurological manifestations. Three patients presented with acute kidney injury and eight patients had coinfection with malaria. Fever with nausea and vomiting was the most common presentation. About 15% of patients presented with bleeding manifestations. About 40.6% of patients presenting as abdominal manifestations had platelet count <20,000/mm3 and needed platelet transfusion versus 9.8% with other system involvement (central nervous system, cardiovascular system (CVS), renal). Hepatomegaly was the most common ultrasonography (USG) finding being present in 57.5% of patients followed by acalculous cholecystitis in 21.3%. Total mortality was 1.9% in our series. We lost eight patients presenting with neurological manifestations and two patients with coinfection with malaria.
Conclusion: Atypical presentations should prompt us to investigate for dengue especially during ongoing epidemics so that expanded dengue syndrome can be diagnosed and treated early.
Keywords: Acalculous cholecystitis; expanded dengue syndrome; transaminitis.
Conflict of interest statement
There are no conflicts of interest.
Figures

Similar articles
-
Sociodemographic and Clinico-laboratory Profile of Expanded Dengue Syndrome: Experience from a Tertiary Hospital of Dhaka, Bangladesh.Mymensingh Med J. 2021 Oct;30(4):1073-1078. Mymensingh Med J. 2021. PMID: 34605479
-
Unusual manifestations in dengue outbreak 2009, Delhi, India.J Commun Dis. 2010 Dec;42(4):255-61. J Commun Dis. 2010. PMID: 22471194
-
Clinical profile and atypical manifestation of dengue fever cases between 2011 and 2018 in Chennai, India.J Family Med Prim Care. 2020 Feb 28;9(2):1119-1123. doi: 10.4103/jfmpc.jfmpc_926_19. eCollection 2020 Feb. J Family Med Prim Care. 2020. PMID: 32318478 Free PMC article.
-
Expanded Dengue.J Assoc Physicians India. 2016 Jul;64(7):59-63. J Assoc Physicians India. 2016. PMID: 27759344 Review.
-
Unusual Manifestations of Dengue Fever: A Review on Expanded Dengue Syndrome.Cureus. 2020 Sep 27;12(9):e10678. doi: 10.7759/cureus.10678. Cureus. 2020. PMID: 33133844 Free PMC article. Review.
Cited by
-
An Intriguing Case of Expanded Dengue Syndrome With Co-existing Encephalitis, Pancreatitis, and Hepatitis: The Classic Thalamic "Double-Doughnut" Sign Revisited.Neurohospitalist. 2024 Jul;14(3):316-321. doi: 10.1177/19418744241230730. Epub 2024 Jan 28. Neurohospitalist. 2024. PMID: 38894998 Free PMC article.
-
Postdengue chronic fatigue syndrome in an adolescent boy.BMJ Case Rep. 2021 Jun 7;14(6):e238605. doi: 10.1136/bcr-2020-238605. BMJ Case Rep. 2021. PMID: 34099442 Free PMC article.
-
Expanded dengue syndrome presenting with acute liver failure, acute kidney injury, pancreatic involvement, coagulopathy, and multiple intracranial hemorrhages in a young child: a case report.J Med Case Rep. 2022 Mar 29;16(1):123. doi: 10.1186/s13256-022-03348-0. J Med Case Rep. 2022. PMID: 35346359 Free PMC article.
-
Viral characteristics and clinical presentation in dengue co-infection- Findings from a facility based observational study in Odisha, India.J Family Med Prim Care. 2021 Aug;10(8):2958-2963. doi: 10.4103/jfmpc.jfmpc_2380_20. Epub 2021 Aug 27. J Family Med Prim Care. 2021. PMID: 34660431 Free PMC article.
-
Short-term, medium-term, and long-term risks of nonvariceal upper gastrointestinal bleeding after dengue virus infection.PLoS Negl Trop Dis. 2022 Jan 19;16(1):e0010039. doi: 10.1371/journal.pntd.0010039. eCollection 2022 Jan. PLoS Negl Trop Dis. 2022. PMID: 35045094 Free PMC article.
References
-
- WHO Dengue and severe dengue. Fact sheet. WHO; 2017.
-
- Pangtey GS, Prakash A, Munjal YP. Role of Carica papaya leaf extract for dengue associated thrombocytopenia. J Assoc Physicians India. 2016;64:11–3. - PubMed
-
- Kadam DB, Salvi S, Chandanwale A. Expanded dengue. J Assoc Physicians India. 2016;64:59–63. - PubMed
-
- Bhatty S, Shaikh NA, Fatima M, Sumbhuani AK. Acute acalculous cholecystitis in dengue fever. J Pak Assoc. 2009;59:519–21. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
