

Treatment of Infections Due to MDR Gram-Negative Bacteria
- PMID: 31041313
- PMCID: PMC6477053
- DOI: 10.3389/fmed.2019.00074
Treatment of Infections Due to MDR Gram-Negative Bacteria
Abstract
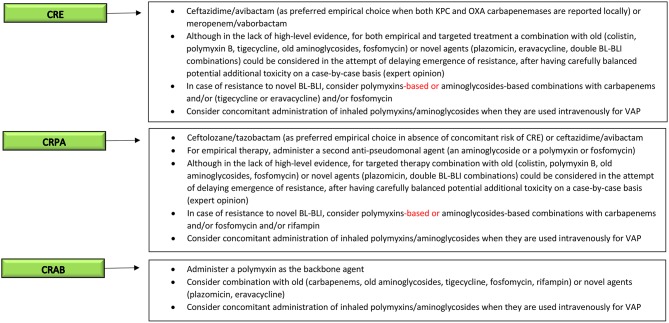
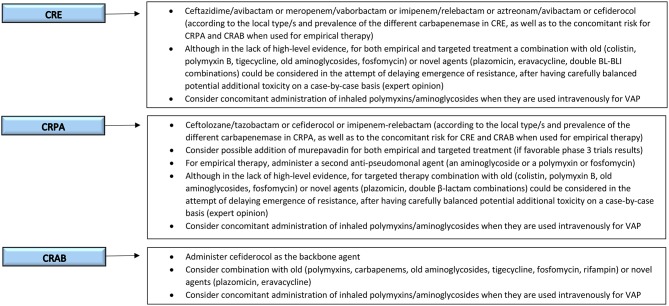
The treatment of multidrug-resistant Gram-negative bacteria (MDR-GNB) infections in critically ill patients presents many challenges. Since an effective treatment should be administered as soon as possible, resistance to many antimicrobial classes almost invariably reduces the probability of adequate empirical coverage, with possible unfavorable consequences. In this light, readily available patient's medical history and updated information about the local microbiological epidemiology remain critical for defining the baseline risk of MDR-GNB infections and firmly guiding empirical treatment choices, with the aim of avoiding both undertreatment and overtreatment. Rapid diagnostics and efficient laboratory workflows are also of paramount importance both for anticipating diagnosis and for rapidly narrowing the antimicrobial spectrum, with de-escalation purposes and in line with antimicrobial stewardship principles. Carbapenem-resistant Enterobacteriaceae, Pseudomonas aeruginosa, and Acinetobacter baumannii are being reported with increasing frequencies worldwide, although with important variability across regions, hospitals and even single wards. In the past few years, new treatment options, such as ceftazidime/avibactam, meropenem/vaborbactam, ceftolozane/tazobactam, plazomicin, and eravacycline have become available, and others will become soon, which have provided some much-awaited resources for effectively counteracting severe infections due to these organisms. However, their optimal use should be guaranteed in the long term, for delaying as much as possible the emergence and diffusion of resistance to novel agents. Despite important progresses, pharmacokinetic/pharmacodynamic optimization of dosages and treatment duration in critically ill patients has still some areas of uncertainty requiring further study, that should take into account also resistance selection as a major endpoint. Treatment of severe MDR-GNB infections in critically ill patients in the near future will require an expert and complex clinical reasoning, of course taking into account the peculiar characteristics of the target population, but also the need for adequate empirical coverage and the more and more specific enzyme-level activity of novel antimicrobials with respect to the different resistance mechanisms of MDR-GNB.
Keywords: Acinetobacter; ICU; Klebsiella; MDR; Pseudomonas; antimicrobial resistance; gram-negative.
Figures
References
-
- Garonzik SM, Li J, Thamlikitkul V, Paterson DL, Shoham S, Jacob J, et al. Population pharmacokinetics of colistin methanesulfonate and formed colistin in critically ill patients from a multicenter study provide dosing suggestions for various categories of patients. Antimicrob Agents Chemother. (2011) 55:3284–94. 10.1128/AAC.01733-10 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous