

Bucindolol for the Maintenance of Sinus Rhythm in a Genotype-Defined HF Population: The GENETIC-AF Trial
- PMID: 31042551
- PMCID: PMC7205445
- DOI: 10.1016/j.jchf.2019.04.004
Bucindolol for the Maintenance of Sinus Rhythm in a Genotype-Defined HF Population: The GENETIC-AF Trial
Abstract
Objectives: The purpose of this study was to compare the effectiveness of bucindolol with that of metoprolol succinate for the maintenance of sinus rhythm in a genetically defined heart failure (HF) population with atrial fibrillation (AF).
Background: Bucindolol is a beta-blocker whose unique pharmacologic properties provide greater benefit in HF patients with reduced ejection fraction (HFrEF) who have the beta1-adrenergic receptor (ADRB1) Arg389Arg genotype.
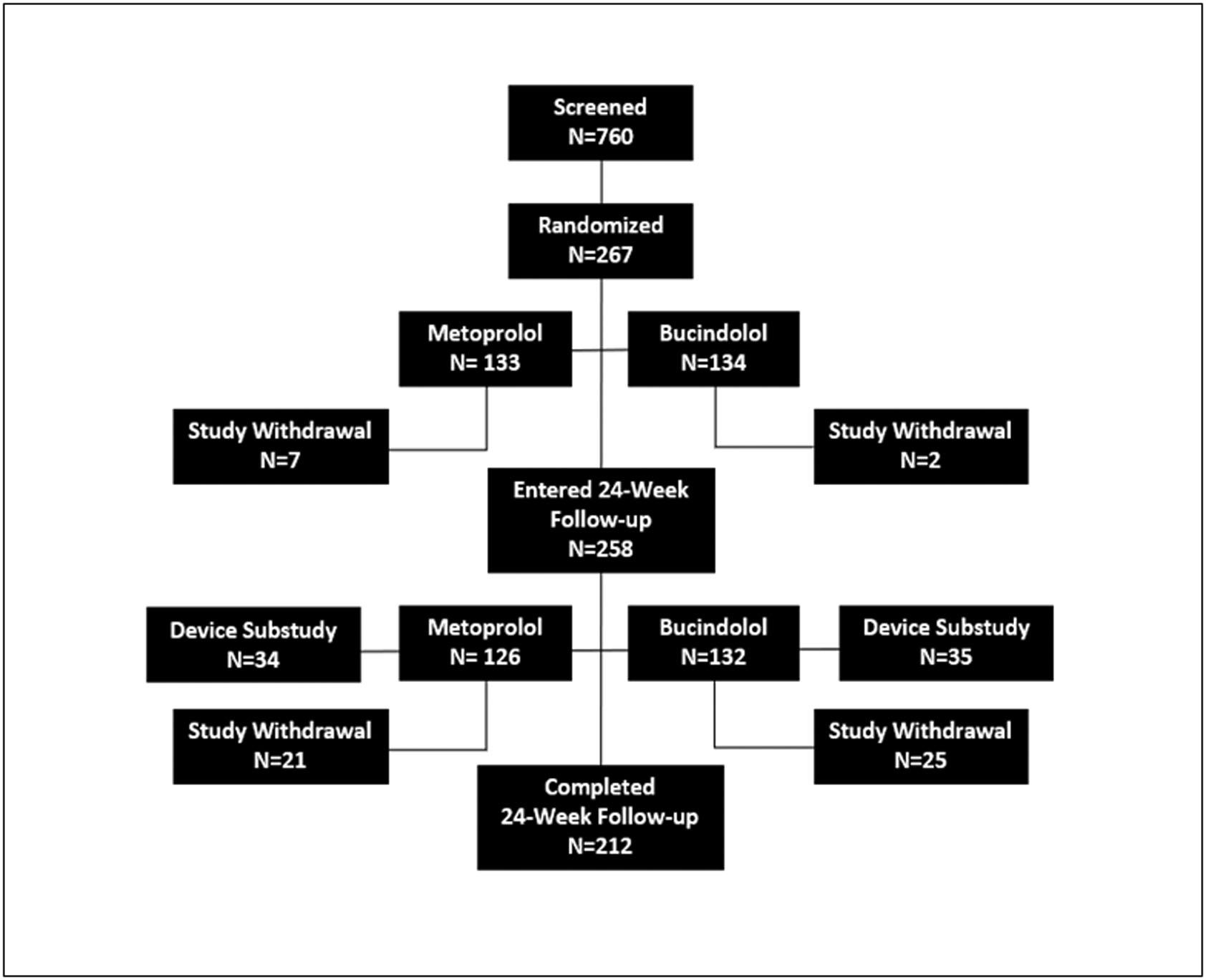
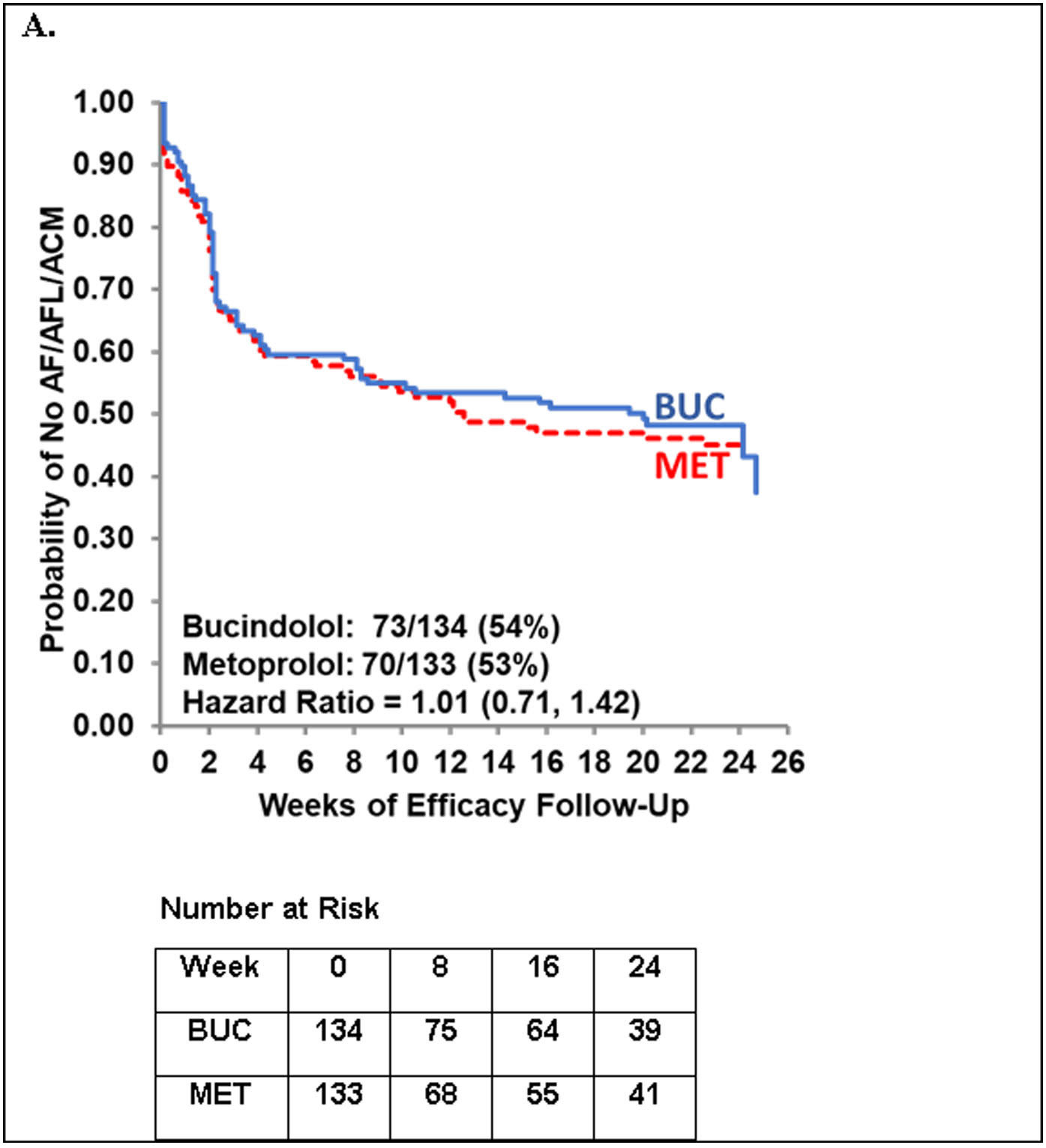
Methods: A total of 267 HFrEF patients with a left ventricular ejection fraction (LVEF) <0.50, symptomatic AF, and the ADRB1 Arg389Arg genotype were randomized 1:1 to receive bucindolol or metoprolol therapy and were up-titrated to target doses. The primary endpoint of AF or atrial flutter (AFL) or all-cause mortality (ACM) was evaluated by electrocardiogram (ECG) during a 24-week period.
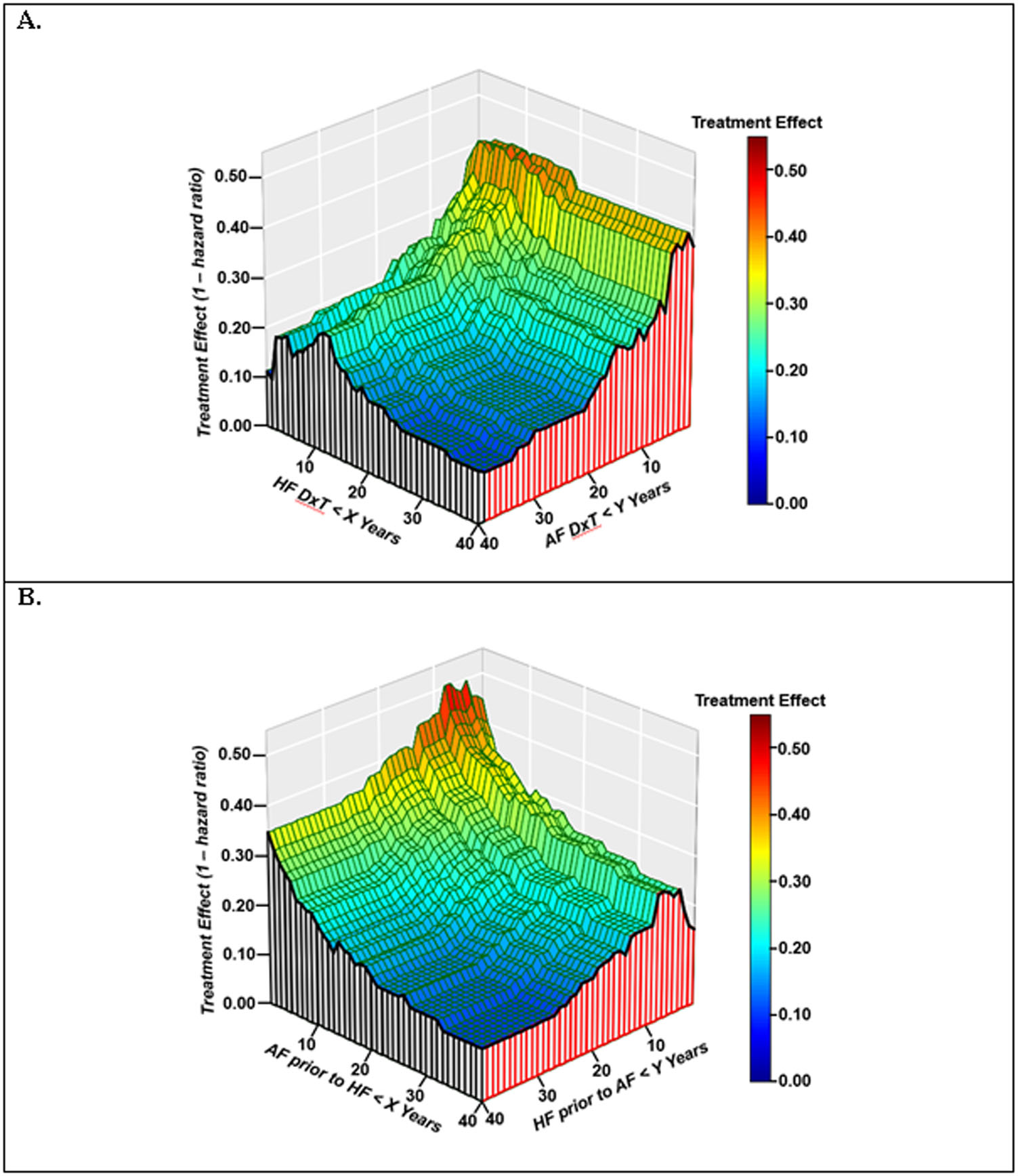
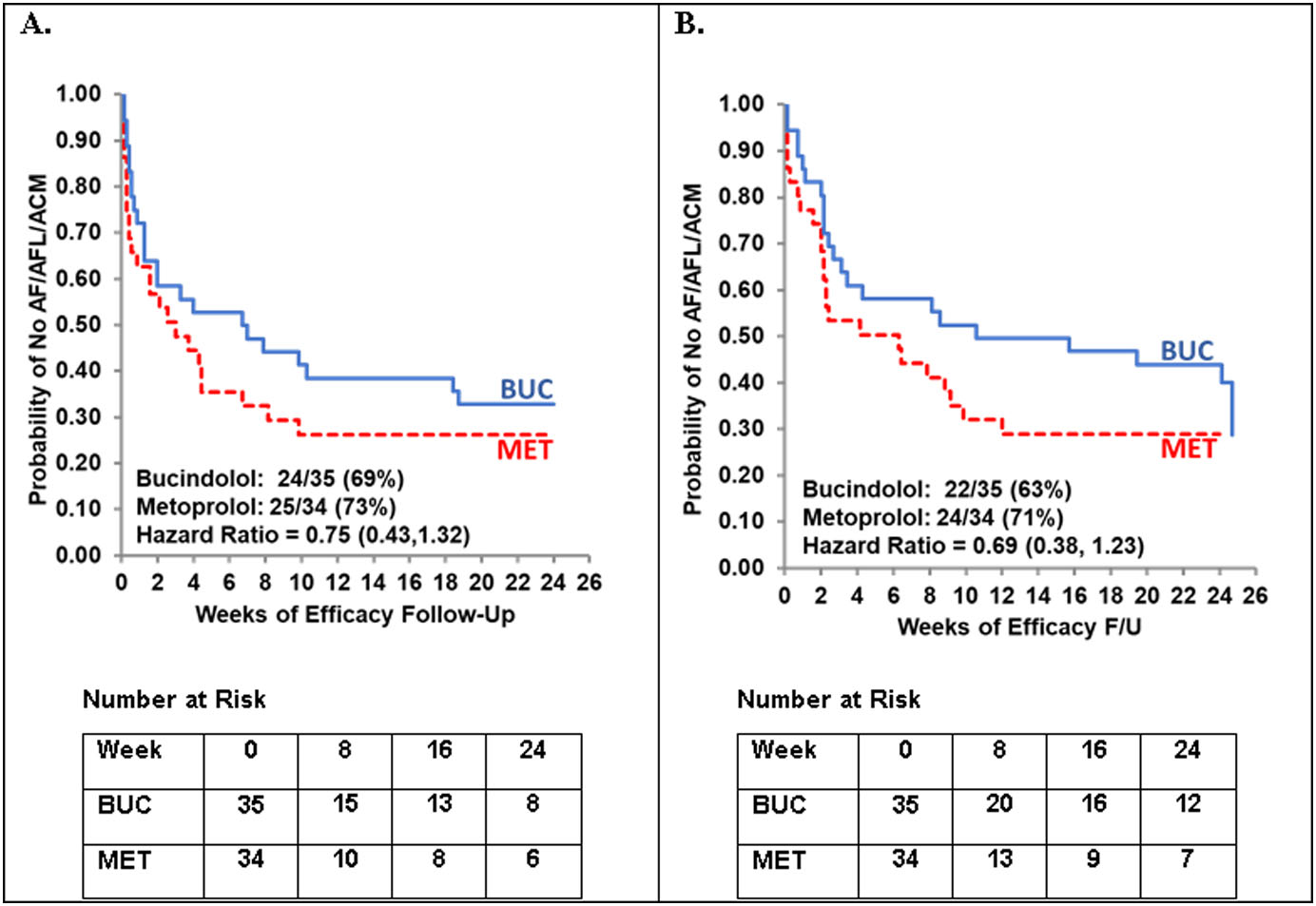
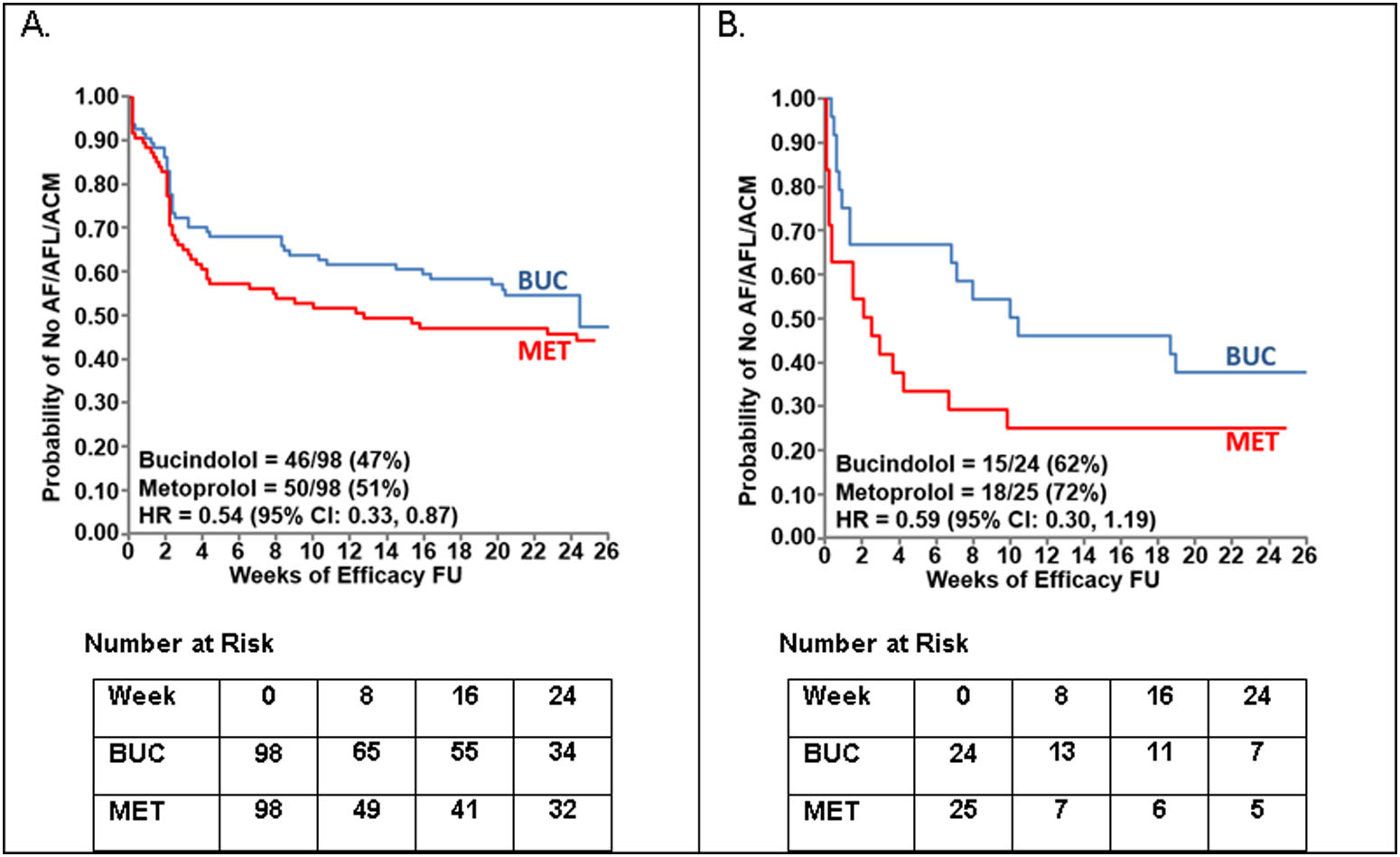
Results: The hazard ratio (HR) for the primary endpoint was 1.01 (95% confidence interval [CI]: 0.71 to 1.42), but trends for bucindolol benefit were observed in several subgroups. Precision therapeutic phenotyping revealed that a differential response to bucindolol was associated with the interval of time from the initial diagnoses of AF and HF to randomization and with the onset of AF relative to that of the initial HF diagnosis. In a cohort whose first AF and HF diagnoses were <12 years prior to randomization, in which AF onset did not precede HF by more than 2 years (n = 196), the HR was 0.54 (95% CI: 0.33 to 0.87; p = 0.011).
Conclusions: Pharmacogenetically guided bucindolol therapy did not reduce the recurrence of AF/AFL or ACM compared to that of metoprolol therapy in HFrEF patients, but populations were identified who merited further investigation in future phase 3 trials.
Keywords: atrial fibrillation; beta-blocker; bucindolol; heart failure; pharmacogenetics; precision medicine.
Copyright © 2019. Published by Elsevier Inc.
Figures
Comment in
-
GENETIC-AF: Digging Deeper Into Genotype-Phenotype and Heart Failure-Atrial Fibrillation Interactions.JACC Heart Fail. 2019 Jul;7(7):599-601. doi: 10.1016/j.jchf.2019.05.005. JACC Heart Fail. 2019. PMID: 31248570 No abstract available.
References
-
- Trulock KM, Narayan SM, Piccini JP. Rhythm control in heart failure patients with atrial fibrillation: contemporary challenges including the role of ablation. J Am Coll Cardiol 2014;64:710–21. - PubMed
-
- Olsson LG, Swedberg K, Ducharme A et al. Atrial fibrillation and risk of clinical events in chronic heart failure with and without left ventricular systolic dysfunction: results from the Candesartan in Heart failure-Assessment of Reduction in Mortality and morbidity (CHARM) program. J Am Coll Cardiol 2006;47:1997–2004. - PubMed
-
- Wang TJ, Larson MG, Levy D et al. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation 2003;107:2920–5. - PubMed
-
- Turagam MK, Garg J, Whang W et al. Catheter Ablation of Atrial Fibrillation in Patients With Heart Failure: A Meta-analysis of Randomized Controlled Trials. Ann Intern Med. 2019;170(1):41–50.. - PubMed
-
- Marrouche NF, Brachmann J, Andresen D et al. Catheter Ablation for Atrial Fibrillation with Heart Failure. N Engl J Med 2018;378:417–427. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
