

Comparison of injury severity scores (ISS) obtained by manual coding versus "Two-step conversion" from ICD-9-CM
- PMID: 31042768
- PMCID: PMC6493742
- DOI: 10.1371/journal.pone.0216206
Comparison of injury severity scores (ISS) obtained by manual coding versus "Two-step conversion" from ICD-9-CM
Abstract
Background: The International Classification of Diseases (ICD) is the standard diagnostic tool for classifying and coding diseases and injuries. The Abbreviated Injury Scale (AIS) is the most widely used injury severity scoring system. Although manual coding is considered the gold standard, it is sometimes unavailable or impractical. There have been many prior attempts to develop programs for the automated conversion of ICD rubrics into AIS codes.
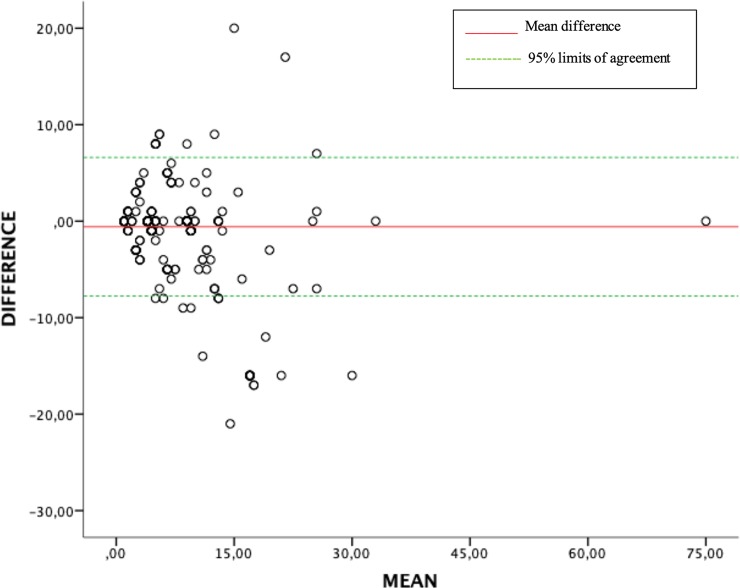
Objective: To convert ICD, Ninth Revision, Clinical Modification (ICD-9-CM) codes into AIS 2005 (update 2008) codes via a derived map using a two-step process and, subsequently, to compare Injury Severity Score (ISS) resulting from said conversion with manually coded ISS values.
Methods: A cross-sectional retrospective study was designed in which medical records at the Hospital Universitario Marqués de Valdecilla of Cantabria (HUMV) and the Complejo Hospitalario of Navarra (CHN), both in Spain, were reviewed. Coding of injuries using AIS 2005 (update 2008) version was done manually by a certified AIS specialist and ISS values were calculated. ICD-9-CM codes were automatically converted into ISS values by another certified AIS specialist in a two-step process. ISS scores obtained from manual coding were compared to those obtained through this conversion process.
Results: The comparison of obtained through conversion versus manual ISS resulted in 396 concordant pairs (70.2%); the analysis of values according to ISS categories (ISS<9, ISS 9-15, ISS 16-24, ISS>24) showed 493 concordant pairs (87.4%). Regarding the criterion of "major trauma" patient (i.e., ISS> 15), 538 matching pairs (95.2%) were obtained. The conversion process resulted in underestimation of ISS in 112 cases (19.9%) and conversion was not possible in 136 cases (19%) for different reasons.
Conclusions: The process used in this study has proven to be a useful tool for selecting patients who meet the ISS>15 criterion for "major trauma". Further research is needed to improve the conversion process.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- AAAM. Escala de Lesiones Abreviada 2005. Actualización 2008. Association for the Advancement for Automotive Medicine ed. Illinois:DesPlaines: AAAM; 2008.
-
- The injury severity score: development and potential usefulness. Proceedings: American Association for Automotive Medicine Annual Conference: Association for the Advancement of Automotive Medicine; 1974.
-
- Osler T, Baker SP, Long W. A modification of the injury severity score that both improves accuracy and simplifies scoring. Journal of Trauma and Acute Care Surgery 1997;43(6):922–926. - PubMed
-
- European Commission, Directorate-General for Internal Market, Industry, Entrepreneurship and SMEs. REPORT FROM THE COMMISSION TO THE EUROPEAN PARLIAMENT AND THE COUNCIL Saving Lives: Boosting Car Safety in the EU Reporting on the monitoring and assessment of advanced vehicle safety features, their cost effectiveness and feasibility for the review of the regulations on general vehicle safety and on the protection of pedestrians and other vulnerable road users. 2016;COM/2016/0787 final.
-
- Zonfrillo MR, Weaver AA, Gillich PJ, Price JP, Stitzel JD. New methodology for an expert-designed map from International Classification of Diseases (ICD) to Abbreviated Injury Scale (AIS) 3 severity injury. Traffic injury prevention 2015;16(sup2):S197–S200. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
