

Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma
- PMID: 31042825
- PMCID: PMC8202968
- DOI: 10.1056/NEJMoa1817226
Anti-BCMA CAR T-Cell Therapy bb2121 in Relapsed or Refractory Multiple Myeloma
Abstract
Background: Preclinical studies suggest that bb2121, a chimeric antigen receptor (CAR) T-cell therapy that targets B-cell maturation antigen (BCMA), has potential for the treatment of multiple myeloma.
Methods: In this phase 1 study involving patients with relapsed or refractory multiple myeloma, we administered bb2121 as a single infusion at doses of 50×106, 150×106, 450×106, or 800×106 CAR-positive (CAR+) T cells in the dose-escalation phase and 150×106 to 450×106 CAR+ T cells in the expansion phase. Patients had received at least three previous lines of therapy, including a proteasome inhibitor and an immunomodulatory agent, or were refractory to both drug classes. The primary end point was safety.
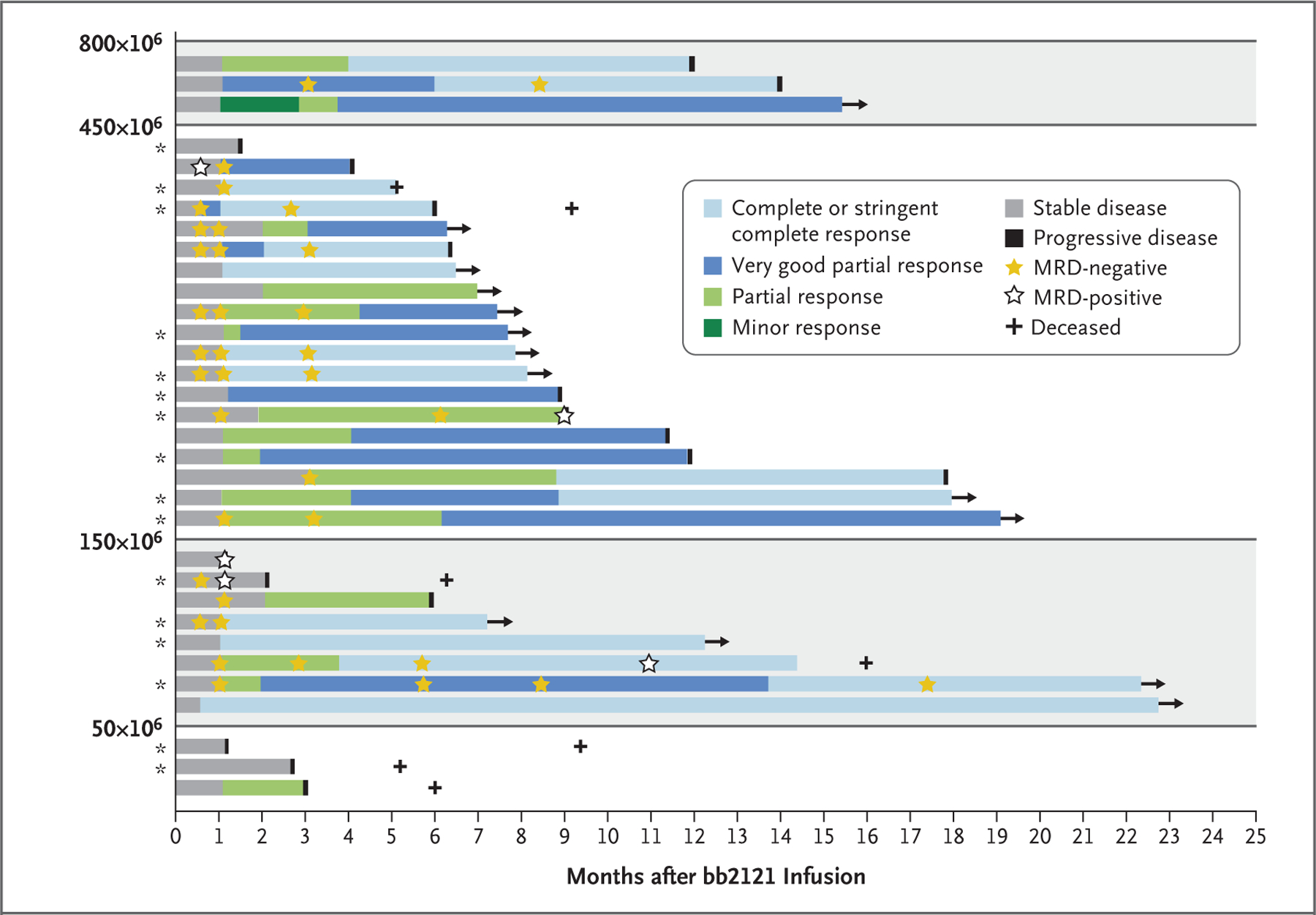
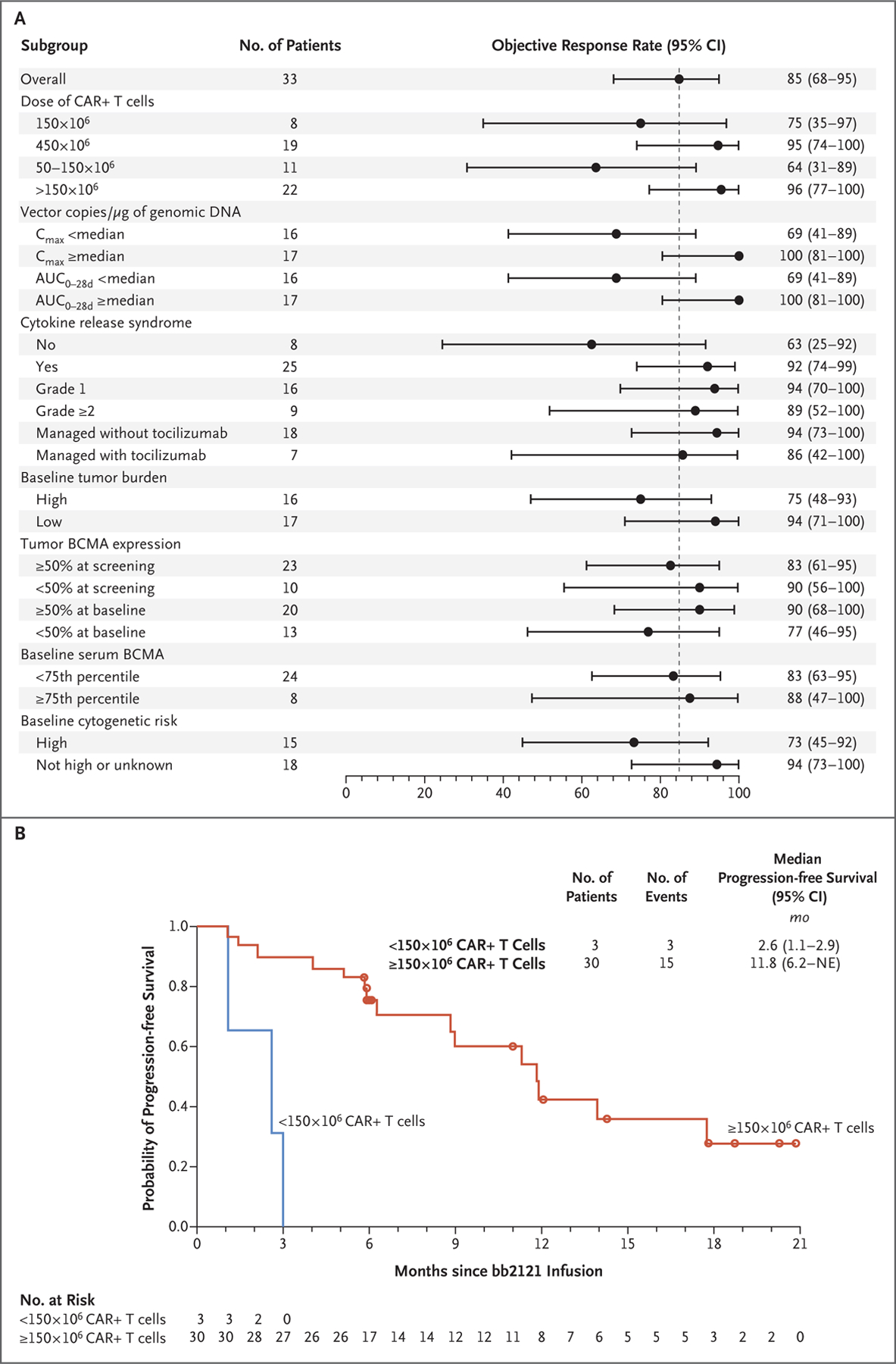
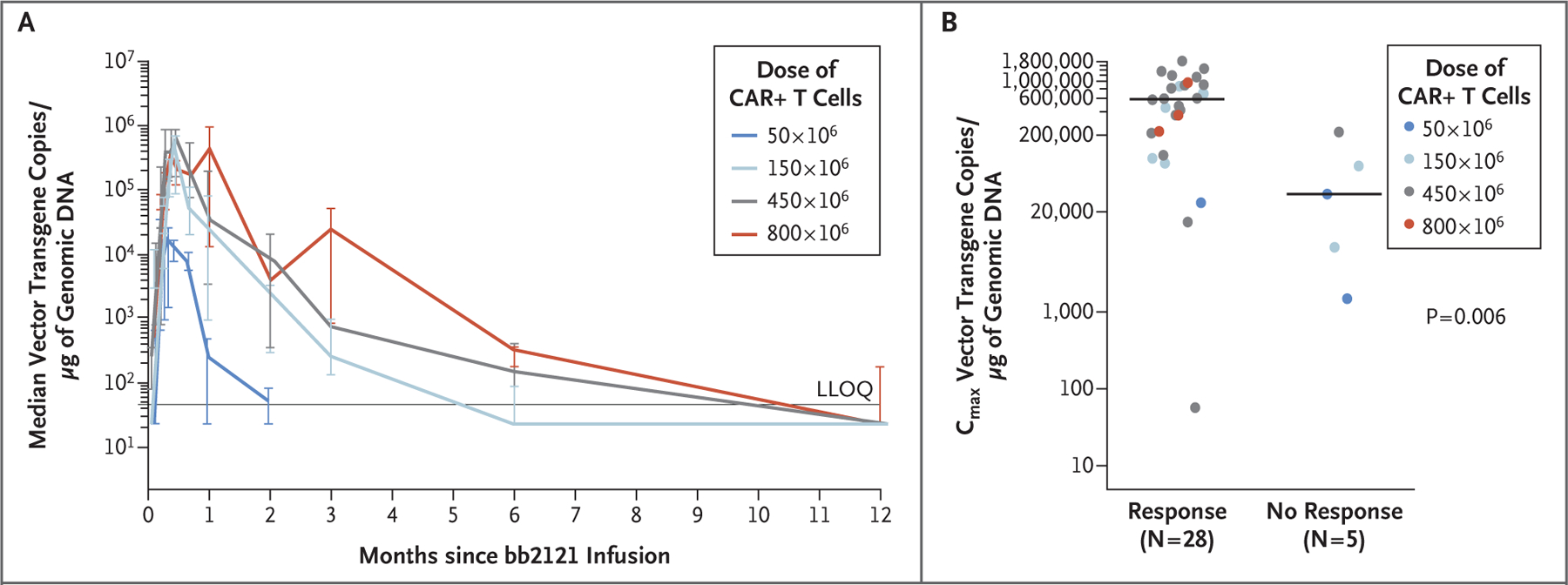
Results: Results for the first 33 consecutive patients who received a bb2121 infusion are reported. The data-cutoff date was 6.2 months after the last infusion date. Hematologic toxic effects were the most common events of grade 3 or higher, including neutropenia (in 85% of the patients), leukopenia (in 58%), anemia (in 45%), and thrombocytopenia (in 45%). A total of 25 patients (76%) had cytokine release syndrome, which was of grade 1 or 2 in 23 patients (70%) and grade 3 in 2 patients (6%). Neurologic toxic effects occurred in 14 patients (42%) and were of grade 1 or 2 in 13 patients (39%). One patient (3%) had a reversible grade 4 neurologic toxic effect. The objective response rate was 85%, including 15 patients (45%) with complete responses. Six of the 15 patients who had a complete response have had a relapse. The median progression-free survival was 11.8 months (95% confidence interval, 6.2 to 17.8). All 16 patients who had a response (partial response or better) and who could be evaluated for minimal residual disease (MRD) had MRD-negative status (≤10-4 nucleated cells). CAR T-cell expansion was associated with responses, and CAR T cells persisted up to 1 year after the infusion.
Conclusions: We report the initial toxicity profile of a BCMA-directed cellular immunotherapy for patients with relapsed or refractory multiple myeloma. Antitumor activity was documented. (Funded by Bluebird Bio and Celgene; CRB-401 ClinicalTrials.gov number, NCT02658929.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
CAR T-cell therapy for relapsed or refractory multiple myeloma.Lancet Oncol. 2019 Jun;20(6):e297. doi: 10.1016/S1470-2045(19)30288-8. Epub 2019 May 10. Lancet Oncol. 2019. PMID: 31085047 No abstract available.
-
Anti-BCMA CAR T cells for MM.Nat Rev Clin Oncol. 2019 Aug;16(8):465. doi: 10.1038/s41571-019-0229-x. Nat Rev Clin Oncol. 2019. PMID: 31089270 No abstract available.
-
Anti-BCMA CAR T-cell Therapy Reins in Myeloma.Cancer Discov. 2019 Jul;9(7):818-819. doi: 10.1158/2159-8290.CD-NB2019-063. Epub 2019 Jun 4. Cancer Discov. 2019. PMID: 31164342
-
Anti-BCMA CAR T-Cell Therapy in Multiple Myeloma.N Engl J Med. 2019 Jul 18;381(3):e6. doi: 10.1056/NEJMc1907520. N Engl J Med. 2019. PMID: 31314981 No abstract available.
References
-
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med 2011;364:1046–60. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials