

Design, implementation, and analysis considerations for cluster-randomized trials in infection control and hospital epidemiology: A systematic review
- PMID: 31043183
- PMCID: PMC6897299
- DOI: 10.1017/ice.2019.48
Design, implementation, and analysis considerations for cluster-randomized trials in infection control and hospital epidemiology: A systematic review
Abstract
Background: In cluster-randomized trials (CRT), groups rather than individuals are randomized to interventions. The aim of this study was to present critical design, implementation, and analysis issues to consider when planning a CRT in the healthcare setting and to synthesize characteristics of published CRT in the field of healthcare epidemiology.
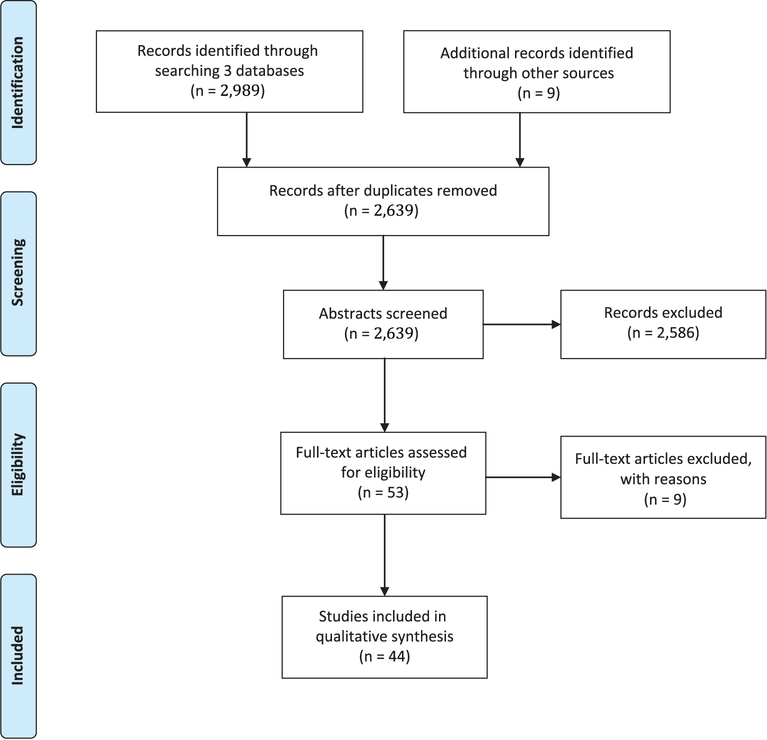
Methods: A systematic review was conducted to identify CRT with infection control outcomes.
Results: We identified the following 7 epidemiological principles: (1) identify design type and justify the use of CRT; (2) account for clustering when estimating sample size and report intraclass correlation coefficient (ICC)/coefficient of variation (CV); (3) obtain consent; (4) define level of inference; (5) consider matching and/or stratification; (6) minimize bias and/or contamination; and (7) account for clustering in the analysis. Among 44 included studies, the most common design was CRT with crossover (n = 15, 34%), followed by parallel CRT (n = 11, 25%) and stratified CRT (n = 7, 16%). Moreover, 22 studies (50%) offered justification for their use of CRT, and 20 studies (45%) demonstrated that they accounted for clustering at the design phase. Only 15 studies (34%) reported the ICC, CV, or design effect. Also, 15 studies (34%) obtained waivers of consent, and 7 (16%) sought consent at the cluster level. Only 17 studies (39%) matched or stratified at randomization, and 10 studies (23%) did not report efforts to mitigate bias and/or contamination. Finally, 29 studies (88%) accounted for clustering in their analyses.
Conclusions: We must continue to improve the design and reporting of CRT to better evaluate the effectiveness of infection control interventions in the healthcare setting.
Conflict of interest statement
Figures
References
-
- Donner A, Klar N. Design and Analysis of Cluster Randomization Trials in Health Research. London: Arnold, 2000.
-
- Moberg J, Kramer M. A brief history of the cluster randomized trial design. JLL Bulletin: Commentaries on the history of treatment evaluation. James Lind Library website. http://www.jameslindlibrary.org/articles/a-brief-history-of-the-cluster-.... Published 2015. Accessed March 8, 2019.
-
- Hayes RJ, Alexander ND, Bennett S, Cousens SN. Design and analysis issues in cluster-randomized trials of interventions against infectious diseases. Statist Method Med Res 2000;9:95–116. - PubMed
-
- Wolkewitz M, Barnett AG, Martinez MP, Frank U, Schumacher M, IMPLEMENT Study Group. Interventions to control nosocomial infections: study designs and statistical issues. J Hosp Infect 2014;86:77–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
