

Small intestinal microbial dysbiosis underlies symptoms associated with functional gastrointestinal disorders
- PMID: 31043597
- PMCID: PMC6494866
- DOI: 10.1038/s41467-019-09964-7
Small intestinal microbial dysbiosis underlies symptoms associated with functional gastrointestinal disorders
Abstract
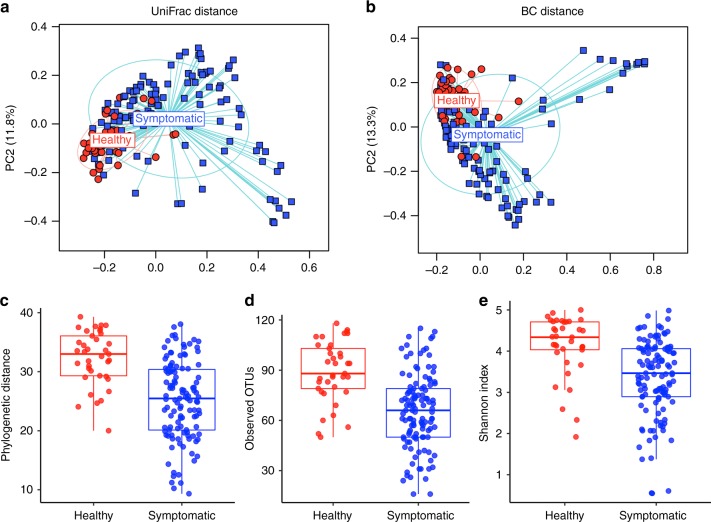
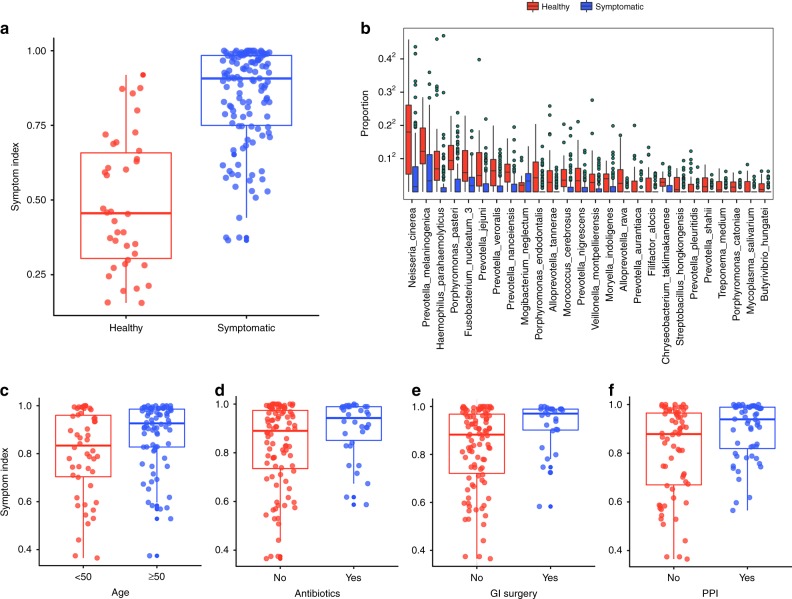
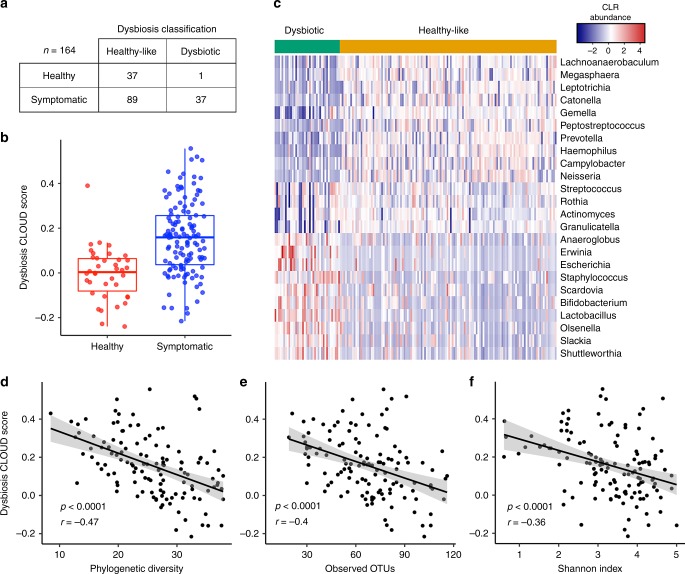
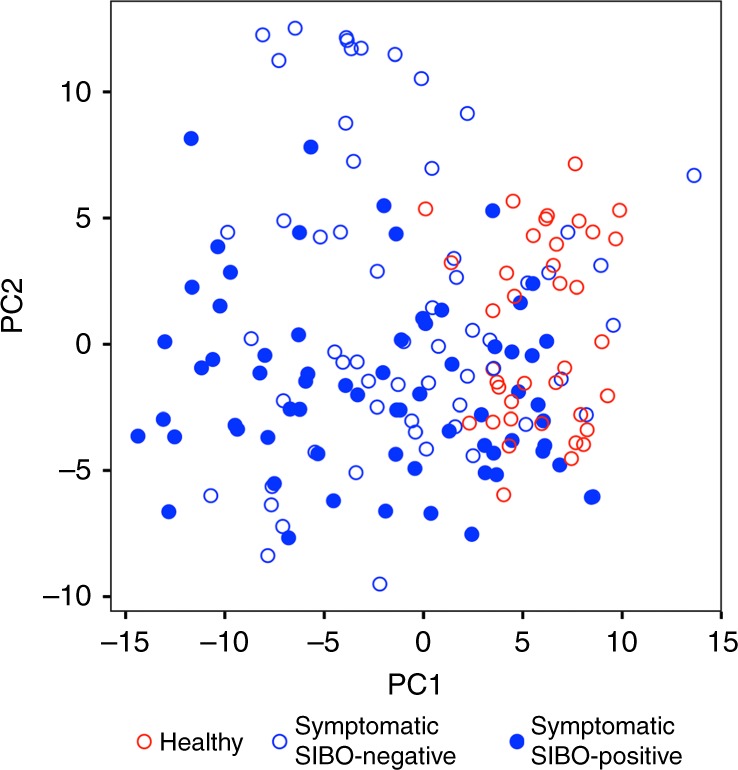
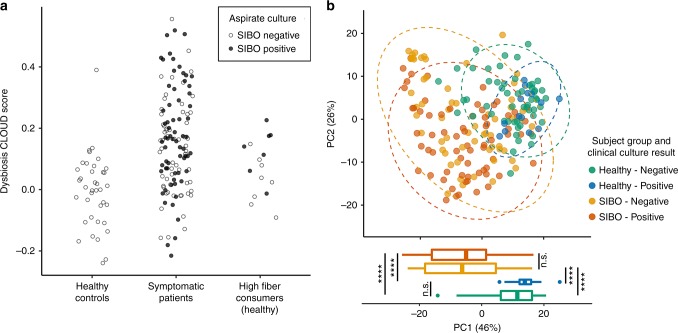
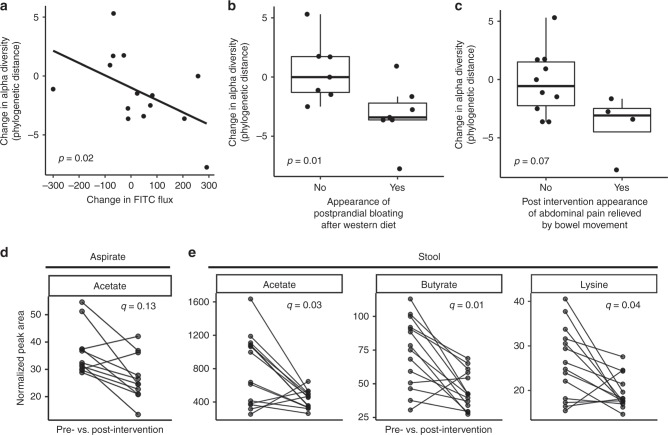
Small intestinal bacterial overgrowth (SIBO) has been implicated in symptoms associated with functional gastrointestinal disorders (FGIDs), though mechanisms remain poorly defined and treatment involves non-specific antibiotics. Here we show that SIBO based on duodenal aspirate culture reflects an overgrowth of anaerobes, does not correspond with patient symptoms, and may be a result of dietary preferences. Small intestinal microbial composition, on the other hand, is significantly altered in symptomatic patients and does not correspond with aspirate culture results. In a pilot interventional study we found that switching from a high fiber diet to a low fiber, high simple sugar diet triggered FGID-related symptoms and decreased small intestinal microbial diversity while increasing small intestinal permeability. Our findings demonstrate that characterizing small intestinal microbiomes in patients with gastrointestinal symptoms may allow a more targeted antibacterial or a diet-based approach to treatment.
Conflict of interest statement
Robin Patel: Dr. Patel reports grants from CD Diagnostics, BioFire, Curetis, Merck, Hutchison Biofilm Medical Solutions, Accelerate Diagnostics, Allergan, and The Medicines Company. Dr. Patel is or has been a consultant to Curetis, Specific Technologies, Selux Dx, GenMark Diagnostics, PathoQuest, Heraeus Medical and Genentech; monies are paid to Mayo Clinic. In addition, Dr. Patel has a patent on
Figures
Comment in
-
Symptoms and the small intestinal microbiome - the unknown explored.Nat Rev Gastroenterol Hepatol. 2019 Aug;16(8):457-458. doi: 10.1038/s41575-019-0171-5. Nat Rev Gastroenterol Hepatol. 2019. PMID: 31213706 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
