

Cervical Pessary versus Expectant Management for the Prevention of Delivery Prior to 36 Weeks in Women with Placenta Previa: A Randomized Controlled Trial
- PMID: 31044098
- PMCID: PMC6491366
- DOI: 10.1055/s-0039-1687871
Cervical Pessary versus Expectant Management for the Prevention of Delivery Prior to 36 Weeks in Women with Placenta Previa: A Randomized Controlled Trial
Abstract
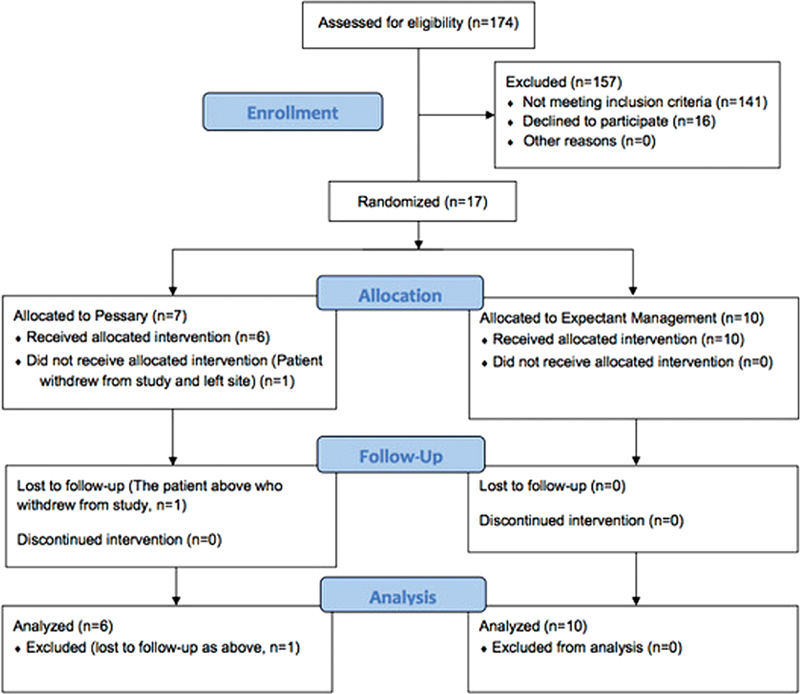
Objective This multicenter randomized controlled trial compared cervical pessary (CP) versus expectant management (EM) in women with placenta previa between 22.0 and 32.0 in prolonging gestation until ≥ 36.0 weeks' gestation. Study Design This study took place from November 2016 to June 2018. Women were randomized to receive either the Bioteque CP or EM. The pessary was removed at ≥ 36.0 weeks unless indicated. The primary outcome was gestational age (GA) at delivery, with secondary outcomes including need for transfusion, number and duration of antepartum admissions, type of delivery, and neonatal outcomes. A total of 140 patients were needed to show a 3-week prolongation of pregnancy in the pessary group; however, the trial was stopped early due to budgetary issues. Results Of the 33 eligible women, 17 were enrolled. Although not statistically significant, the mean GA at delivery in the CP group was greater than women in the EM group (36.5 ± 1.23 vs. 36.0 ± 2.0; p = 0.1673). The number and duration of antepartum admissions was greater in the EM group (2.7 ± 0.58 vs. 16.0 ± 22.76 days; p = 0.1264) as well. Conclusion Although the study was underpowered to determine the primary outcome, safety and feasibility of CP in pregnancies complicated with previa were demonstrated.
Keywords: hemorrhage; pessary; placenta previa; preterm birth.
Conflict of interest statement
Figures
References
-
- Silver R M. Abnormal placentation: placenta previa, vasa previa, and placenta accreta. Obstet Gynecol. 2015;126(03):654–668. - PubMed
-
- Iyasu S, Saftlas A K, Rowley D L, Koonin L M, Lawson H W, Atrash H K. The epidemiology of placenta previa in the United States, 1979 through 1987. Am J Obstet Gynecol. 1993;168(05):1424–1429. - PubMed
-
- Cresswell J A, Ronsmans C, Calvert C, Filippi V. Prevalence of placenta praevia by world region: a systematic review and meta-analysis. Trop Med Int Health. 2013;18(06):712–724. - PubMed
-
- Getahun D, Oyelese Y, Salihu H M, Ananth C V. Previous cesarean delivery and risks of placenta previa and placental abruption. Obstet Gynecol. 2006;107(04):771–778. - PubMed
-
- Ananth C V, Smulian J C, Vintzileos A M. The association of placenta previa with history of cesarean delivery and abortion: a metaanalysis. Am J Obstet Gynecol. 1997;177(05):1071–1078. - PubMed