Analysis of Control Arm Quality in Randomized Clinical Trials Leading to Anticancer Drug Approval by the US Food and Drug Administration
- PMID: 31046071
- PMCID: PMC6499129
- DOI: 10.1001/jamaoncol.2019.0167
Analysis of Control Arm Quality in Randomized Clinical Trials Leading to Anticancer Drug Approval by the US Food and Drug Administration
Erratum in
-
Errors in Data Presentation in Text, Figures, Table, and eTables.JAMA Oncol. 2019 Aug 1;5(8):1232. doi: 10.1001/jamaoncol.2019.2422. JAMA Oncol. 2019. PMID: 31219519 Free PMC article. No abstract available.
Abstract
Importance: To date, an empirical evaluation of the quality of control arms in randomized clinical trials (RCTs) leading to anticancer drug approvals by the US Food and Drug Administration (FDA) has not been undertaken.
Objective: We sought to estimate the percentage of RCTs that used a control arm deemed suboptimal and led to FDA approval of anticancer drugs from January 1, 2013, to July 31, 2018.
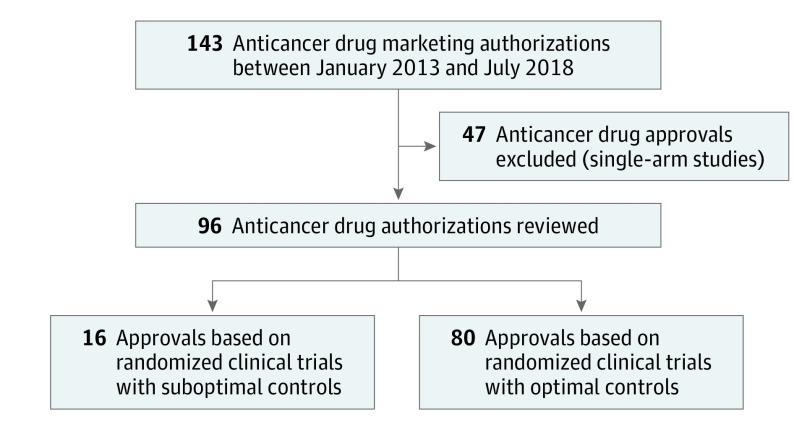
Design, setting, and participants: This quality improvement study included 143 anticancer drug approvals granted by the FDA from January 1, 2013, to July 31, 2018. All approvals based on single-arm studies (48 approvals) were excluded. Approvals based on RCTs were further investigated and each trial was analyzed for design, time of patient accrual, control arm, and primary end point. Standard-of-care therapy was determined by evaluating the literature and published guidelines 1 year prior to the start of trial enrollment. The percentage of approvals based on RCTs that used suboptimal control arms was then calculated. The quality of the control arm was deemed suboptimal if the choice of control agent was restricted to exclude a recommended agent, the control arm was specified but the recommended agent was unspecified, and if prior RCT data had demonstrated that the control agent was inferior to an available alternative.
Main outcomes and measures: Estimated percentage of RCTs that used suboptimal control arms that led to FDA approval of anticancer agents between January 1, 2013, to July 31, 2018.
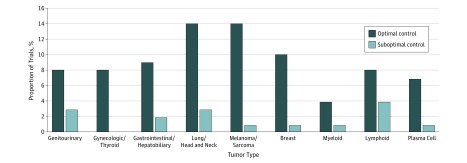
Results: A total of 145 studies that led to 143 drug approvals between January 1, 2013, and July 31, 2018, were included. Of these studies, 48 single-arm studies were excluded. The remaining 97 studies led to 95 drug approvals. Of these 95 approvals, 16 (17%) were based on RCTs with suboptimal control arms; 15 were international trials, and 1 was conducted in the United States. The type of approval was regular in 15 trials and accelerated in 1 trial. When categorized by the nature of suboptimal control, 4 (25%) trials omitted active treatment in control arm by limiting investigator's choice, 11 (63%) trials omitted active treatment in the control arm by using a control agent known to be inferior to other available agents or not allowing combinations, and 1 (13%) trial used a previously used treatment in the control arm with a known lack of benefit associated with reexposure.
Conclusions and relevance: Although anticancer drug approvals are increasing, a proportion of these drugs are reaching the market without proven superiority to what is considered the standard of care at the time of patient enrollment in pivotal trials. The choice of control arm should be optimized to ensure that new anticancer agents being marketed are truly superior to what most clinicians would prescribe outside a clinical trial setting.
Conflict of interest statement
Figures