

Contralateral ovarian endometrioma recurrence after unilateral salpingo-oophorectomy
- PMID: 31046768
- PMCID: PMC6498560
- DOI: 10.1186/s12905-019-0760-z
Contralateral ovarian endometrioma recurrence after unilateral salpingo-oophorectomy
Abstract
Background: The recurrence rate after unilateral salpingo-oophorectomy (USO) for unilateral endometrioma has not been reported. We evaluated the rate of and risk factors for endometrioma recurrence after USO.
Methods: In this retrospective observational study, we enrolled 110 women (age, 35-45 years) who underwent laparoscopic USO (n = 50) or cystectomy (n = 60) for unilateral ovarian endometrioma from January 2010 through December 2012. We compared patients' characteristics between patients who underwent USO and those who underwent cystectomy. We also compared patients with and without an endometrioma recurrence after USO using univariate and multivariate stepwise logistic regression models to identify recurrence risk factors. Endometrioma recurrence was defined as an ovarian cyst (> 2 cm) with features typical of an endometrioma identified by postoperative transvaginal sonography.
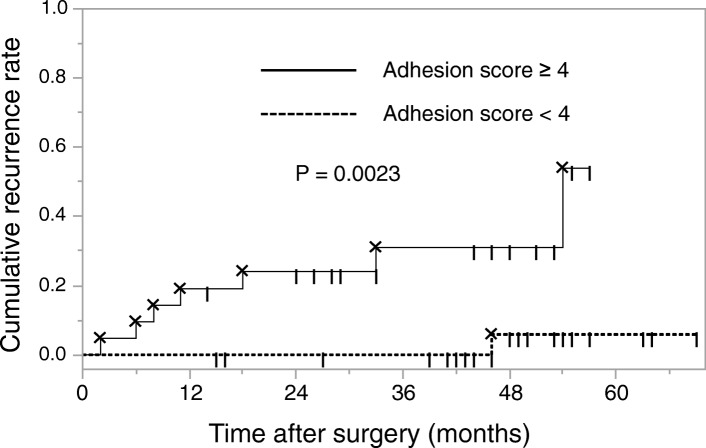
Results: Endometrioma recurred in 8 (16%) patients after USO (mean follow-up, 46.0 ± 12.9 months [range, 15-73]). The post-USO cumulative recurrence rates at 12, 24, 36, and 60 months were 8.0, 10.2, 12.7, and 24.7%, respectively (Kaplan-Meier analysis). In logistic regression analysis, a contralateral side adhesion score ≥ 4 was an independent risk factor for endometrioma recurrence after USO (odds ratio, 19.48, 95% confidence interval, 1.59-237.72). The post-USO cumulative recurrence rates at 12, 24, 36, and 57 months were 19.5, 24.1, 31.0, and 54.0%, respectively, in cases with contralateral side adhesion scores ≥4, and 0.0, 0.0, 0.0, and 5.9%, respectively, in cases with scores < 4 (log-rank test, P = 0.0023).
Conclusions: To our knowledge, this is the first report on the recurrence rate and risk factors associated with recurrence after USO. Endometrioma recurrence rates were 24.7% during the first 5 years after USO. The post-USO recurrence rate increased significantly in cases with contralateral side adhesions. Our findings could improve the planning of USO and patient selection for postoperative hormonal therapy.
Keywords: Endometriosis; Recurrence; Unilateral endometrioma; Unilateral salpingo-oophorectomy.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of Tokyo University Hospital. We obtained written informed consent from all participants before surgery.
Consent for publication
All participants provided written informed consent to publish the information.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Recurrence rate of endometrioma after laparoscopic cystectomy: a comparative randomized trial between post-operative hormonal suppression treatment or dietary therapy vs. placebo.Eur J Obstet Gynecol Reprod Biol. 2009 Nov;147(1):72-7. doi: 10.1016/j.ejogrb.2009.07.003. Epub 2009 Aug 7. Eur J Obstet Gynecol Reprod Biol. 2009. PMID: 19665279 Clinical Trial.
-
Salpingo-oophorectomy or surveillance for ovarian endometrioma in asymptomatic premenopausal women: a cost-effectiveness analysis.Am J Obstet Gynecol. 2022 Aug;227(2):311.e1-311.e7. doi: 10.1016/j.ajog.2022.04.043. Epub 2022 Apr 28. Am J Obstet Gynecol. 2022. PMID: 35490792
-
Recurrence of ovarian endometrioma after second-line, conservative, laparoscopic cyst enucleation.Am J Obstet Gynecol. 2014 Mar;210(3):216.e1-6. doi: 10.1016/j.ajog.2013.11.007. Epub 2013 Nov 8. Am J Obstet Gynecol. 2014. PMID: 24215855
-
Conservative surgery in ovarian borderline tumours: a meta-analysis with emphasis on recurrence risk.Eur J Cancer. 2015 Mar;51(5):620-31. doi: 10.1016/j.ejca.2015.01.004. Epub 2015 Feb 3. Eur J Cancer. 2015. PMID: 25661104 Review.
-
Salpingo-oophorectomy versus cystectomy in patients with borderline ovarian tumors: a systemic review and meta-analysis on postoperative recurrence and fertility.World J Surg Oncol. 2021 Apr 21;19(1):132. doi: 10.1186/s12957-021-02241-2. World J Surg Oncol. 2021. PMID: 33882931 Free PMC article.
Cited by
-
Pyroptotic T cell-derived active IL-16 has a driving function in ovarian endometriosis development.Cell Rep Med. 2024 Mar 19;5(3):101476. doi: 10.1016/j.xcrm.2024.101476. Cell Rep Med. 2024. PMID: 38508138 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
