

Quantitative pupillometry for the monitoring of intracranial hypertension in patients with severe traumatic brain injury
- PMID: 31046817
- PMCID: PMC6498599
- DOI: 10.1186/s13054-019-2436-3
Quantitative pupillometry for the monitoring of intracranial hypertension in patients with severe traumatic brain injury
Abstract
Background: Elevated intracranial pressure (ICP) is frequent after traumatic brain injury (TBI) and may cause abnormal pupillary reactivity, which in turn is associated with a worse prognosis. Using automated infrared pupillometry, we examined the relationship between the Neurological Pupil index (NPi) and invasive ICP in patients with severe TBI.
Methods: This was an observational cohort of consecutive subjects with severe TBI (Glasgow Coma Scale [GCS] < 9 with abnormal lesions on head CT) who underwent parenchymal ICP monitoring and repeated NPi assessment with the NPi-200® pupillometer. We examined NPi trends over time (four consecutive measurements over intervals of 6 h) prior to sustained elevated ICP > 20 mmHg. We further analyzed the relationship of cumulative abnormal NPi burden (%NPi values < 3 during total ICP monitoring time) with intracranial hypertension (ICHT)-categorized as refractory (ICHT-r; requiring surgical decompression) vs. non-refractory (ICHT-nr; responsive to medical therapy)-and with the 6-month Glasgow Outcome Score (GOS).
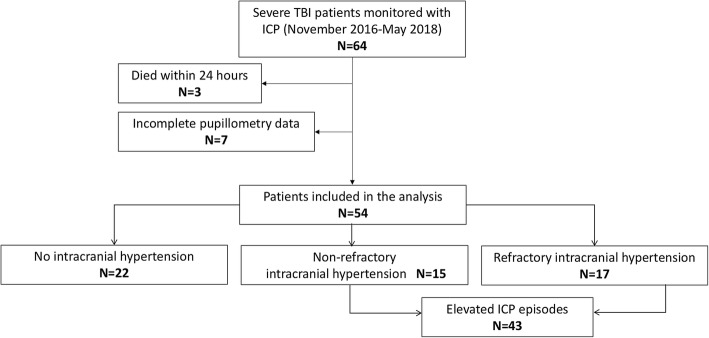
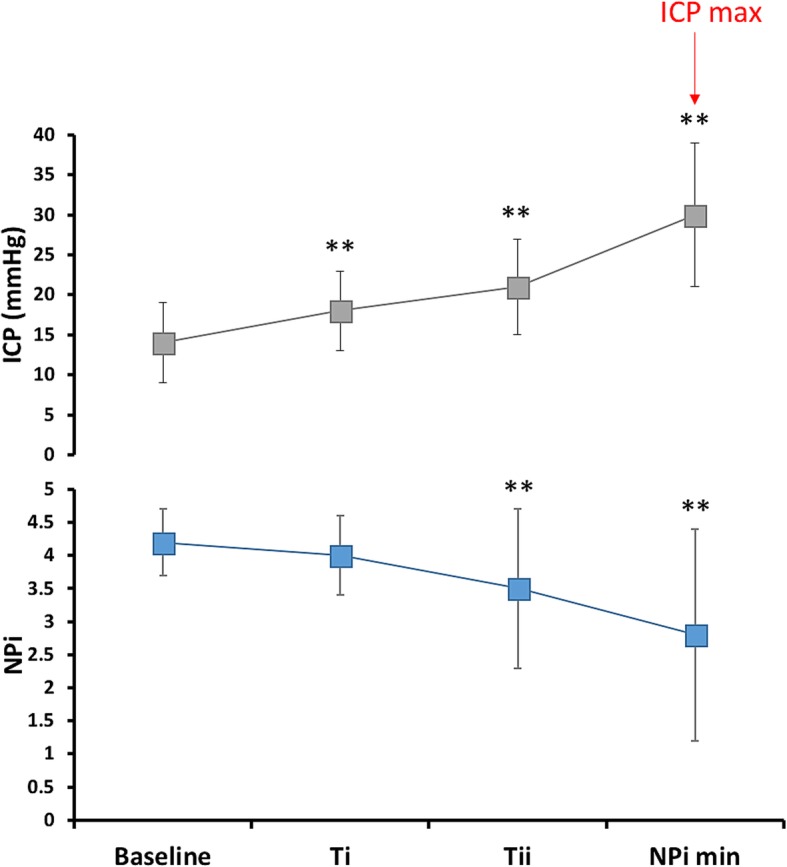
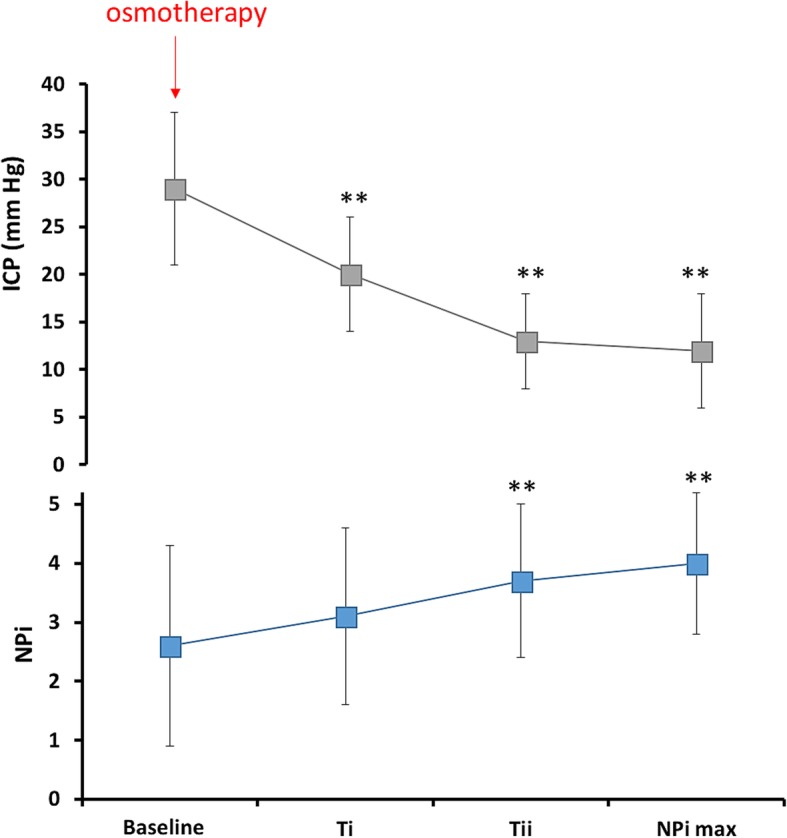
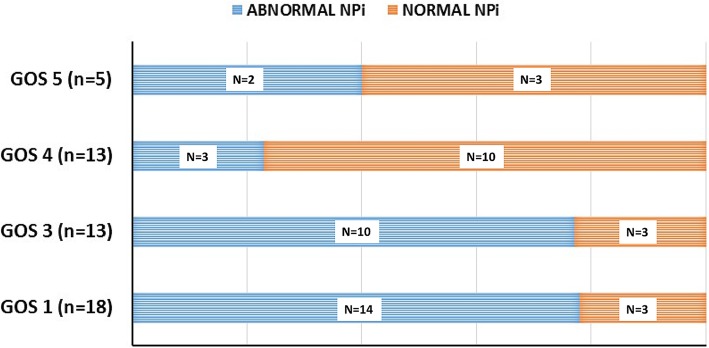
Results: A total of 54 patients were studied (mean age 54 ± 21 years, 74% with focal injuries on CT), of whom 32 (59%) had ICHT. Among subjects with ICHT, episodes of sustained elevated ICP (n = 43, 172 matched ICP-NPi samples; baseline ICP [T- 6 h] 14 ± 5 mmHg vs. ICPmax [T0 h] 30 ± 9 mmHg) were associated with a concomitant decrease of the NPi (baseline 4.2 ± 0.5 vs. 2.8 ± 1.6, p < 0.0001 ANOVA for repeated measures). Abnormal NPi values were more frequent in patients with ICHT-r (n = 17; 38 [3-96]% of monitored time vs. 1 [0-9]% in patients with ICHT-nr [n = 15] and 0.5 [0-10]% in those without ICHT [n = 22]; p = 0.007) and were associated with an unfavorable 6-month outcome (15 [1-80]% in GOS 1-3 vs. 0 [0-7]% in GOS 4-5 patients; p = 0.002).
Conclusions: In a selected cohort of severe TBI patients with abnormal head CT lesions and predominantly focal cerebral injury, elevated ICP episodes correlated with a concomitant decrease of NPi. Sustained abnormal NPi was in turn associated with a more complicated ICP course and worse outcome.
Keywords: Intracranial hypertension; Intracranial pressure; Neurological Pupil index; Outcome; Prognosis; Pupillary reactivity; Pupillometry; Traumatic brain injury.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the ethical committee of the University of Lausanne, with a waiver of consent provided, given the retrospective observational design.
Consent for publication
Not applicable.
Competing interests
Mauro Oddo has received speaker honoraria from Neuroptics®. All the remaining authors declare that they have no competing interest related to this study. The device manufacturer (Neuroptics, Laguna Hills, CA, USA) did not provide any financial support for the study and had no role in the study design, data collection, analysis and interpretation, or writing of the report.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Cnossen MC, Huijben JA, van der Jagt M, Volovici V, van Essen T, Polinder S, Nelson D, Ercole A, Stocchetti N, Citerio G, et al. Variation in monitoring and treatment policies for intracranial hypertension in traumatic brain injury: a survey in 66 neurotrauma centers participating in the CENTER-TBI study. Crit Care. 2017;21(1):233. doi: 10.1186/s13054-017-1816-9. - DOI - PMC - PubMed
-
- Sharshar T, Citerio G, Andrews PJ, Chieregato A, Latronico N, Menon DK, Puybasset L, Sandroni C, Stevens RD. Neurological examination of critically ill patients: a pragmatic approach. Report of an ESICM expert panel. Intensive Care Med. 2014;40(4):484–495. doi: 10.1007/s00134-014-3214-y. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
