

Postdialysis Hypokalemia and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis
- PMID: 31048327
- PMCID: PMC6556735
- DOI: 10.2215/CJN.07950718
Postdialysis Hypokalemia and All-Cause Mortality in Patients Undergoing Maintenance Hemodialysis
Abstract
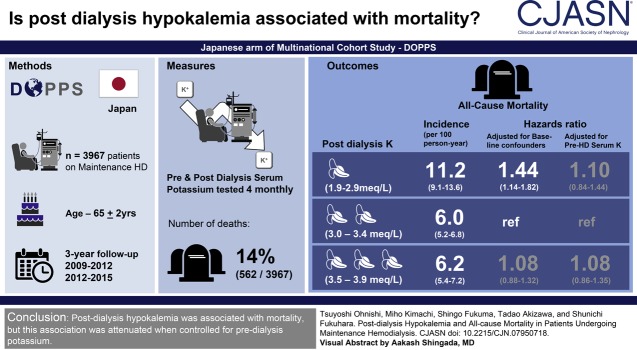
Background and objectives: Almost half of patients on dialysis demonstrate a postdialysis serum potassium ≤3.5 mEq/L. We aimed to examine the relationship between postdialysis potassium levels and all-cause mortality.
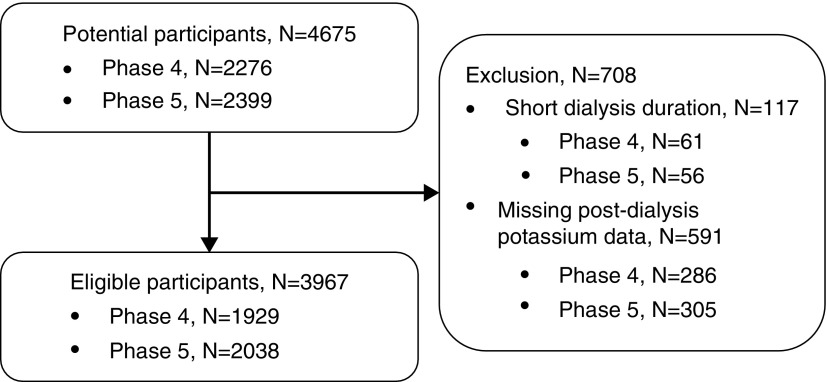
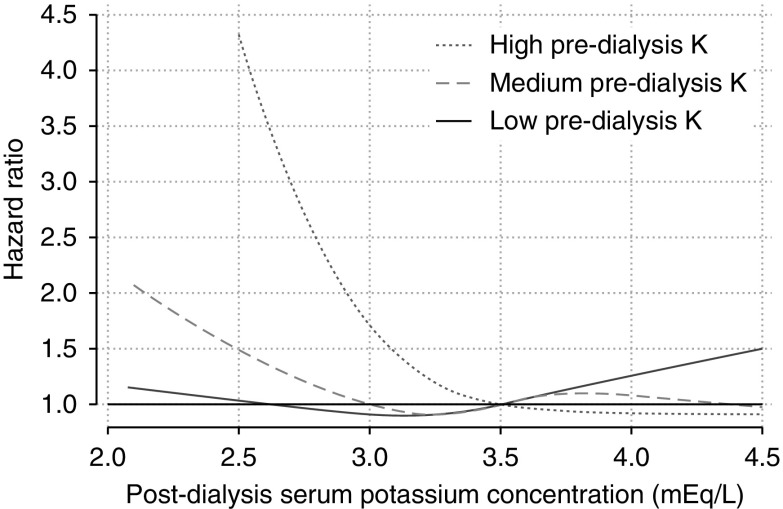
Design, setting, patients, & measurements: We conducted a cohort study of 3967 participants on maintenance hemodialysis from the Dialysis Outcomes and Practice Patterns Study in Japan (2009-2012 and 2012-2015). Postdialysis serum potassium was measured repeatedly at 4-month intervals and used as a time-varying variable. We estimated the hazard ratio of all-cause mortality rate using Cox hazard regression models, with and without adjusting for time-varying predialysis serum potassium. Models were adjusted for baseline characteristics and time-varying laboratory parameters. We also analyzed associations of combinations of pre- and postdialysis potassium with mortality.
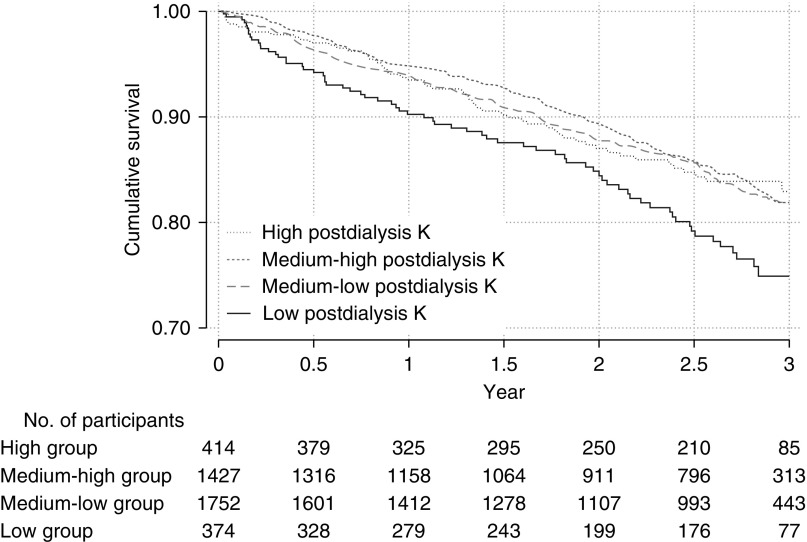
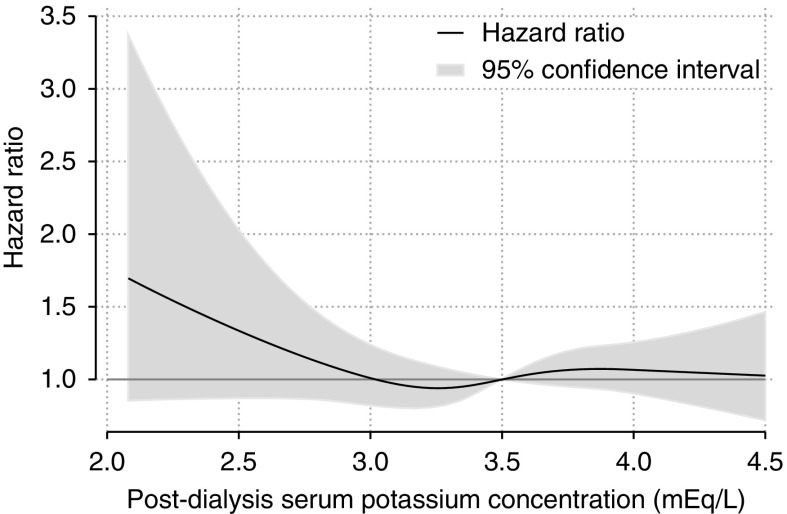
Results: The age of participants at baseline was 65±12 years (mean±SD), 2552 (64%) were men, and 96% were treated with a dialysate potassium level of 2.0 to <2.5 mEq/L. The median follow-up period was 2.6 (interquartile range, 1.3-2.8) years. During the follow-up period, 562 (14%) of 3967 participants died, and the overall mortality rate was 6.7 per 100 person-years. Compared with postdialysis potassium of 3.0 to <3.5 mEq/L, the hazard ratios of postdialysis hypokalemia (<3.0 mEq/L) were 1.84 (95% confidence interval, 1.44 to 2.34) in the unadjusted model, 1.44 (95% confidence interval, 1.14 to 1.82) in the model without adjusting for predialysis serum potassium, and 1.10 (95% confidence interval, 0.84 to 1.44) in the model adjusted for predialysis serum potassium. The combination of pre- and postdialysis hypokalemia was associated with the highest mortality risk (hazard ratio, 1.72; 95% confidence interval, 1.35 to 2.19, reference; pre- and postdialysis nonhypokalemia).
Conclusions: Postdialysis hypokalemia was associated with mortality, but this association was not independent of predialysis potassium.
Keywords: Confidence Intervals; Dialysis Solutions; Follow-Up Studies; Japan-Dialysis Outcomes and Practice Patterns Study; Potassium; Proportional Hazards Models; chronic hemodialysis; electrolytes; end-stage renal disease; hypokalemia; mortality; post-dialysis; renal dialysis; serum potassium.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- United States Renal Data System : 2017 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2017
-
- Kovesdy CP, Regidor DL, Mehrotra R, Jing J, McAllister CJ, Greenland S, Kopple JD, Kalantar-Zadeh K: Serum and dialysate potassium concentrations and survival in hemodialysis patients. Clin J Am Soc Nephrol 2: 999–1007, 2007 - PubMed
-
- Yusuf AA, Hu Y, Singh B, Menoyo JA, Wetmore JB: Serum potassium levels and mortality in hemodialysis patients: A retrospective cohort study. Am J Nephrol 44: 179–186, 2016 - PubMed
-
- Hwang JC, Wang CT, Chen CA, Chen HC: Hypokalemia is associated with increased mortality rate in chronic hemodialysis patients. Blood Purif 32: 254–261, 2011 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
